
COMMUNITY DIGEST
Eight featured cases, twelve quick consultations, and a beta launch. Here is what the EndoCollab community discussed from February 18 through March 6, 2026.
Featured Cases
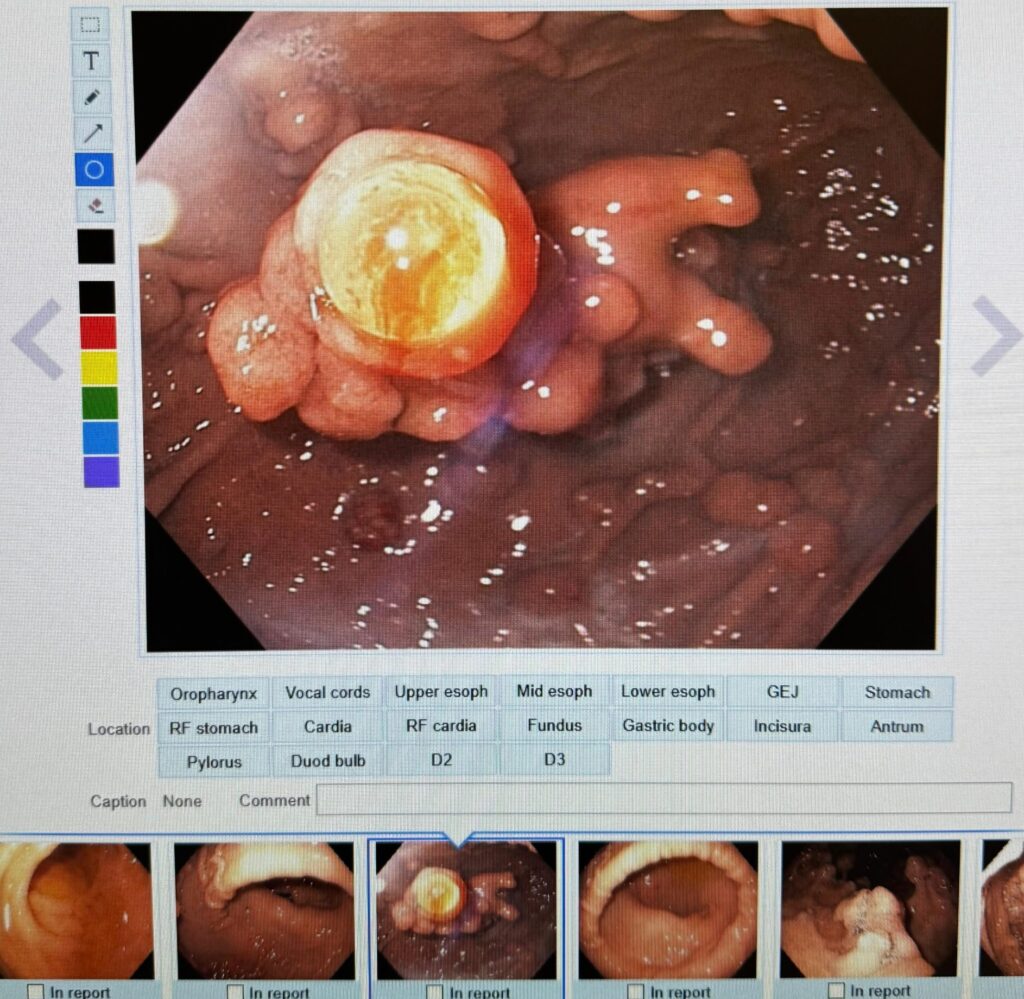
1. Gastric Polyposis With Antral Intussusception: Could This Be GAPPS?
A 73-year-old woman presented with abdominal pain and gastric antral intussusception. EGD showed polyps carpeting the body, cardia, and fundus, but the antrum was spared. Biopsies returned fundic gland polyps.
The group worked through polyposis syndromes (FAP, Peutz-Jeghers, Cronkhite-Canada) before one member identified the pattern as Gastric Adenocarcinoma and Proximal Polyposis of the Stomach (GAPPS): fundic gland polyposis restricted to the proximal stomach with a spared antrum and no colon polyps. At 73, the patient has passed the peak risk window for GAPPS-associated adenocarcinoma, making the surgery vs. surveillance decision especially nuanced.
 1")
2. Failed Duodenal Bulb NET Resection: What Next?
Follow-up to a previously discussed case. A G1, Ki-67 1% non-functional NET adjacent to the pylorus resisted EMR-L, conventional EMR, and hybrid EMR. The tumor was firm, raising concern about muscularis propria invasion.
The group offered four alternatives: FTRD, endoscopic submucosal tunnel dissection, detachable nylon snare ligation, and underwater EMR. When standard EMR fails for duodenal NETs, a second look at imaging to assess depth of invasion is essential.
 2")
3. Esophagitis Dissecans Superficialis in Alcoholic Cirrhosis
During variceal screening (no varices found), a desquamative esophageal pattern was noted. No DOAC or NSAID use. The group initially focused on the classic DOAC association, but when that was ruled out, alcohol abuse emerged as an underappreciated cause.
Multiple members corroborated seeing similar cases after alcohol ingestion. Comparison cases were shared confirming this as a recognized presentation.
 3")
4. Caustic Ingestion: Zargar IIIB With Airway Compromise
Severe caustic ingestion with Zargar IIIB injury in the distal esophagus and IIB/IIIA in the upper and mid segments. The patient had right-sided lobar infiltrates, vocal cord edema and necrosis, and respiratory compromise.
The group outlined the full management protocol: CT chest, continuous PPI infusion, antibiotics, hydration, analgesics, thoracic surgery standby, ICU monitoring, TPN, and psychiatric assessment if the ingestion was intentional. One member noted that given the oropharyngeal status, advancing past the UES would not have been advisable. Update: the patient showed slight respiratory improvement by March 1.
5. Rectal Lesion: Hyperplastic, Serrated, or Ectopic Gastric Mucosa?
A rectal lesion with uncertain endoscopic appearance. Initial reads favored hyperplastic or serrated sessile lesion. One member offered a different interpretation: ectopic gastric mucosa in the rectum, a rare finding that can cause rectal bleeding.
Two PubMed references were shared, including a published case report by a community member. Ectopic gastric mucosa is well known in the esophagus and Meckel’s diverticulum but rarely considered in the rectum.
 4")
6. Gastric Body Findings in Alcoholic With Porcelain Gallbladder
A 50-year-old woman with frequent alcohol use and porcelain gallbladder, presenting with epigastric pain. Endoscopy showed severe erythema with edematous folds, a serpentine mucosal pattern, and whitish areas in the gastric body.
The group discussed portal hypertensive gastropathy, chemical gastritis, and intestinal metaplasia. No hypercalcemia, renal failure, or liver disease was confirmed. The serpentine pattern has a specific differential: PHG, Menetrier’s disease, and lymphocytic gastritis. Whitish areas warrant biopsy to rule out intestinal metaplasia or xanthoma.
 5")
7. MRCP Hilar Discontinuity With Recurrent Pain
Recurrent moderate to severe abdominal pain with normal LFTs and CA 19-9. MRCP showed apparent hilar discontinuity. The group provided an extensive differential: imaging artifact (flow void from the right hepatic artery, respiratory misregistration), vascular compression, anatomic variants, and inflammatory/fibrotic stricture (PSC, IgG4-related disease).
The right hepatic artery crossing the common hepatic duct is the classic cause of apparent biliary discontinuity on MRCP. Always review source images, not just reconstructions. EUS is the right next step.
8. Internal Hemorrhoids With White Anal Mucosa
Internal hemorrhoids with strikingly white mucosal changes. The colorectal surgeon advised against biopsies due to bleeding risk. The group debated leukoplakia, premalignant change, condyloma (HPV), gastric heterotopia, and squamous metaplasia.
Rubber band ligation with simultaneous biopsy was suggested as a practical approach when standalone biopsy carries bleeding concern.
 6")
Quick Cases
February 18
- Ectopic gastric mucosa in duodenum (37-year-old, persistent pain; typically asymptomatic, coeliac disease should be ruled out).
- Hypertrophic anal papilla vs papilloma (quick consensus on hypertrophic anal papilla; argon plasma ablation suggested).
- Capsule endoscopy jejunal lesion (lower GI bleeding history; differential included Meckel’s diverticulum, can be jejunal, not just ileal).
- Esophagogastric junction lesion (severe esophagitis with a finding at the EGJ; discussion centered on intestinal metaplasia at the cardia).
February 21
- RUS vs Crohn’s proctitis (rectal findings with normal colon; isolated anorectal Crohn’s is rare, consider SRUS).
- Crohn’s vs Behcet’s in young male (tofacitinib for sacroileitis with aphthous ulcers and skip lesions; differentiation approach discussed including pathergy test and HLA typing).
- Sphincter of Oddi dysfunction, type 2 (excellent sphincterotomy outcomes reported in women post-cholecystectomy with pain and altered LFTs).
- Antibiotic-dependent pouchitis (UC patient post-colectomy with J pouch; always send stool samples before starting antibiotics).
February 24-27
- Downhill vs uphill varices (spleen size is the differentiator when both types are diffusely large).
March 2
- Recurrent melena in 27-year-old (pancytopenia, jejunal stricture on capsule, proximal jejunal ulcerations; differential includes vasculitis and Crohn’s).
- Gastric lesion, adenomatous? (non-distensible folds, firm on palpation; quick consensus on adenomatous or intestinal dysplastic tissue).
March 3
- Mirizzi syndrome: keep the stent in (the stent serves as an anatomical guide during cholecystectomy and prevents re-obstruction).
March 4
- Rectal polyp EMR with carcinoma in situ (stalk free, resection appears complete; sigmoidoscopy in 6-12 months, colonoscopy in 3 years).
Community Notes
- EndoCollab Case Note Tool: Beta launch. Voice-dictate findings, upload images, get a structured case report as a downloadable PDF.
- A case report was accepted for publication in the March issue of The Practicing Endoscopist.
- Active article exchange throughout the period, with requests typically fulfilled same-day.
What’s Next
- Master GI Bleeding Management — “The Ultimate Guide to GI Bleeding”
- Join EndoCollab — Access our full case library, expert discussions, and continuing education.
