
CASE REPORT
Abstract
Background: Yttrium-90 (Y-90) transarterial radioembolization is an increasingly utilized treatment for unresectable hepatocellular carcinoma. While effective, non-target embolization of microspheres into extrahepatic vessels can result in severe radiation-induced gastrointestinal injury with an incidence of 2–4%.
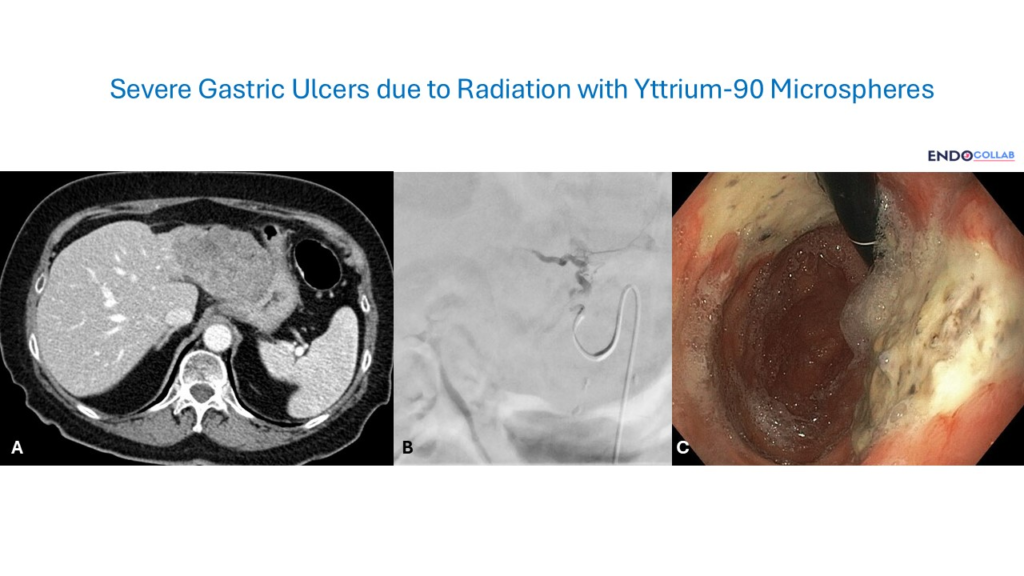
Case: A 75-year-old female with stage IIIC hepatocellular carcinoma developed severe abdominal pain, nausea, vomiting, and weight loss several weeks after Y-90 radioembolization. Esophagogastroduodenoscopy revealed multiple large gastric ulcers in the fundus and proximal body with fibrin-covered bases and visible vessels, consistent with radiation-induced gastric injury.
Conclusion: Y-90 radiation-induced gastric ulcers are characteristically deep, refractory to proton pump inhibitor therapy, and can progress to transmural necrosis, perforation, and sepsis. Recognition of this complication and understanding of its distinct pathophysiology — direct radiogenic microvascular damage rather than acid-related mucosal injury — is essential for appropriate management.
Keywords: Yttrium-90; Y-90 radioembolization; radiation-induced gastric ulcer; hepatocellular carcinoma; non-target embolization; transarterial radioembolization; PPI-refractory ulcer; gastric radiation injury
★ Key Clinical Takeaways
- Non-target embolization of Y-90 microspheres into the gastric vasculature (primarily via the left gastric artery) is the primary mechanism of injury, occurring in 2–4% of cases.
- Symptoms typically present weeks to months after the procedure, making clinical correlation with interventional radiology history essential.
- Endoscopic findings include deep, irregular ulcers with necrotic or fibrin-covered bases, often in the gastric fundus and body.
- These ulcers are characteristically refractory to PPI therapy because the mechanism is radiogenic transmural microvascular damage, not acid-related mucosal injury.
- Severe cases may require surgical intervention due to risk of perforation, hemorrhage, or sepsis.
Clinical History
A 75-year-old female with a history of stage IIIC hepatocellular carcinoma underwent Yttrium-90 selective tumor embolization. The patient had been receiving monoclonal antibody therapy and Y-90 transarterial radioembolization. She presented with severe abdominal pain, nausea, vomiting, and weight loss several weeks after her last embolization, prompting esophagogastroduodenoscopy.

Endoscopic Findings
Esophagogastroduodenoscopy revealed multiple, very large gastric ulcers located in the fundus and proximal body of the stomach. The ulcers were covered by fibrin with necrotic bases and surrounding mucosal erythema. Two areas of visible vessels were noted within the ulcers. No active bleeding was observed during the procedure.
Discussion
Yttrium-90 (Y-90) transarterial radioembolization is an interventional radiology technique used to treat hepatocellular carcinoma and metastatic colon cancer. This therapy is generally considered safe and effective, with increasing utilization over time.
Complications such as duodenal and gastric ulcers have been reported, with an incidence ranging from 2% to 4%. These ulcers result from inadvertent delivery of Y-90 microspheres to the microvasculature of the stomach or duodenum — primarily via the left gastric artery — leading to direct radiation toxicity.
Symptoms, including abdominal pain, weight loss, vomiting, anorexia, and bleeding, typically arise hours to months after therapy. Severe cases of sepsis due to perforation have been reported. Diagnosis is made endoscopically and confirmed histologically.
These radiation-induced gastric ulcers are often recalcitrant to standard proton pump inhibitor therapy due to a distinct pathophysiology: the damage is radiogenic and extends transmurally across the entire thickness of the gastrointestinal tract wall, rather than resulting from acid-mediated mucosal injury. This fundamental difference in mechanism explains the failure of acid suppression and underscores the importance of recognizing this entity as distinct from peptic ulcer disease.
References
- Riaz A, Lewandowski RJ, Kulik LM, et al. Practical management of complications following yttrium-90 radioembolization. Semin Intervent Radiol. 2011;28(4):450–459.
- Hasteh F, Dasyam AK, Kothary N, et al. Gastric and Duodenal Ulceration after Yttrium-90 Radioembolization: Etiology, Clinical Presentation, and Management. J Vasc Interv Radiol. 2017;28(10):1442–1448.
- Kallini JR, Gabr A, Wade T, et al. Complications of Yttrium-90 Radioembolization. Tech Vasc Interv Radiol. 2017;20(2):121–127.
- Mushtaq M et al. Gastric ulcers located with Yttrium-90 microsphere selective internal radiation therapy. Cureus. 2024;16:e58702.
