
CASE REPORT
Abstract
Background: Esophago-pulmonary fistulae are rare but serious complications that may arise following esophagectomy and anastomotic leak in the setting of advanced esophageal carcinoma. Endoscopic stenting offers a palliative alternative when surgical repair is contraindicated.
Case: A 63-year-old male with metastatic esophageal carcinoma developed an esophago-pulmonary fistula following Ivor Lewis esophagectomy complicated by an anastomotic leak. A fully covered self-expanding metal stent was placed under fluoroscopic guidance with external metallic markers to bridge the fistula. The stent was secured using an over-the-scope clip (Stentfix, Ovesco) to prevent migration.
Conclusion: Fully covered self-expanding metal stents anchored with over-the-scope clips provide an effective palliative approach for sealing esophago-pulmonary fistulae, preventing aspiration, and restoring oral intake in patients with limited surgical options.
Keywords: esophago-pulmonary fistula; self-expanding metal stent; fully covered stent; esophageal carcinoma; stent migration; over-the-scope clip; Stentfix; fluoroscopic guidance; palliative endoscopy; esophagectomy complication
★ Key Clinical Takeaways
- Fully covered self-expanding metal stents effectively seal esophago-pulmonary fistulae, preventing aspiration and enabling oral intake in patients who are not surgical candidates.
- External metallic markers (coins, metal bars, or metal pieces) taped to the chest wall and correlated with endoscopic landmarks allow precise fluoroscopic stent positioning.
- Stent migration is a well-recognized complication in esophageal stenting — the Stentfix over-the-scope clip (Ovesco) provides a reliable anchoring method with its open-mouth cap design that secures the stent from both upper and lower tips.
- Confirming guidewire position in the gastric antrum before stent advancement is a critical safety step to prevent malpositioning.
- Aligning internal stent markers with external fluoroscopic markers at deployment ensures adequate coverage of the fistula tract.
Clinical History
A 63-year-old male with a history of metastatic esophageal carcinoma presented following an Ivor Lewis esophagectomy that was complicated by an esophageal anastomotic leak that did not completely heal. Subsequently, the patient developed a new onset tracheoesophageal fistula communicating with the bronchus and pleural space. His disease course was further complicated by extensive metastases to bone and brain, for which he was receiving chemotherapy.
Given the extensive lesion in the soft tissues communicating with the pulmonary space and the patient’s limited surgical candidacy, a decision was made to place a fully covered self-expanding metal stent to bridge this esophago-pulmonary fistula as a palliative intervention.
Endoscopic Findings
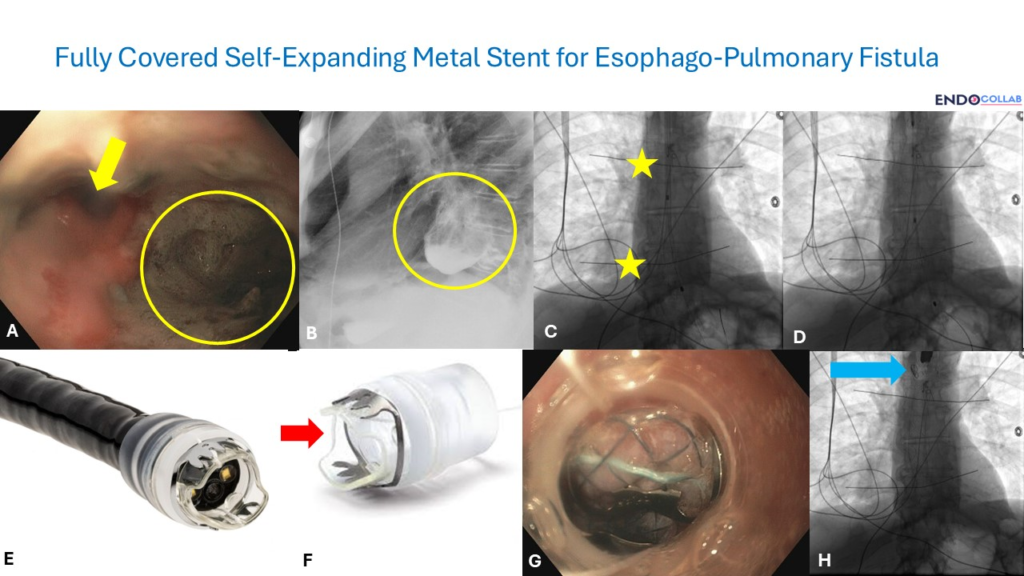
Endoscopic visualization of the esophageal lumen revealed a direct communication to the bronchus and pleura/lung (Figure 1A, yellow arrow and circle). This finding was confirmed by a barium esophagram, which clearly demonstrated the fistulous tract (Figure 1B).

Endoscopic Technique
Fluoroscopy was utilized to guide stent placement. To accurately mark the intended stent location, metallic markers — either a coin, metal bars, or metal pieces — were taped to the upper and lower esophageal landmarks on the chest wall corresponding to the intended stent position. The internal landmark location within the esophagus was correlated with the tip of the endoscope before external marking wire placement. These externally taped metal wires were visualized fluoroscopically (Panel C, yellow stars).
A guidewire was advanced into the stomach, with the distal tip positioned safely in the antrum (Panel D). The endoscope was then removed, leaving the wire in place. A fully covered self-expanding metal stent was advanced over the guidewire under fluoroscopic guidance and deployed when its internal markers aligned with the external fluoroscopic markers at the predetermined location.
To prevent migration into the stomach, the stent was anchored using an over-the-scope clip (Stentfix, Ovesco, USA). This specialized device is a cap preloaded with an over-the-scope clip that is easily advanced into the esophagus (Panel E). The cap features an open-mouth design, allowing both the upper and lower tips to secure the stent (Panel F). The upper part of the stent is held by the lower tip of the cap, while the upper lip of the cap approximates to the esophageal mucosa directly above the stent. The over-the-scope clip was deployed to secure the stent in place (Panel G), with the final result showing the clip holding the fully covered self-expanding metal stent (Panel H).
Discussion
Management of esophago-pulmonary fistulae in patients with advanced metastatic disease poses significant challenges, particularly when surgical repair is contraindicated due to poor overall prognosis or comorbidities. Endoscopic stent placement offers a palliative solution to seal the fistula, allowing for improved quality of life by preventing aspiration and facilitating oral intake.
The use of fully covered self-expanding metal stents is crucial in these cases to ensure complete sealing of the fistula. Unlike partially covered or uncovered stents, the full covering prevents tissue ingrowth through the mesh while maintaining a complete barrier across the fistulous tract.
Stent migration remains a known complication, particularly in the esophagus. Techniques such as anchoring the stent with over-the-scope clips or endoscopic suturing are vital to maintain stent position and ensure long-term efficacy. The Stentfix device used in this case provides a straightforward and effective method for secure stent placement, with its open-mouth design allowing dual fixation to both the stent and adjacent esophageal mucosa.
Fluoroscopic guidance combined with external markers is essential for precise stent deployment to ensure adequate coverage of the fistula and to avoid stent misplacement. The technique of correlating internal endoscopic landmarks with external metallic markers offers a reproducible approach to accurate stent positioning.
References
- Langer FB, Schaefer B, Kulemann B, et al. Esophageal stents in spontaneous esophageal perforations and anastomotic leaks: a single-center experience with 94 patients. Dis Esophagus. 2017;30(3):1-8.
- Van Boeckel PG, Siersema PD. Esophageal stents for benign and malignant diseases. Curr Opin Gastroenterol. 2011;27(4):374-380.
- Sharma P, Kozarek R. Esophageal stenting in the management of benign and malignant conditions. Am J Gastroenterol. 2010;105(3):530-542.
