
COMMUNITY DIGEST
Five featured cases, five quick consultations, and an ERCP cannulation masterclass. Here is what the EndoCollab community discussed from March 7 through March 20, 2026.
Featured Cases
1. Rectal Tonsil vs NET: A Diagnostic Puzzle
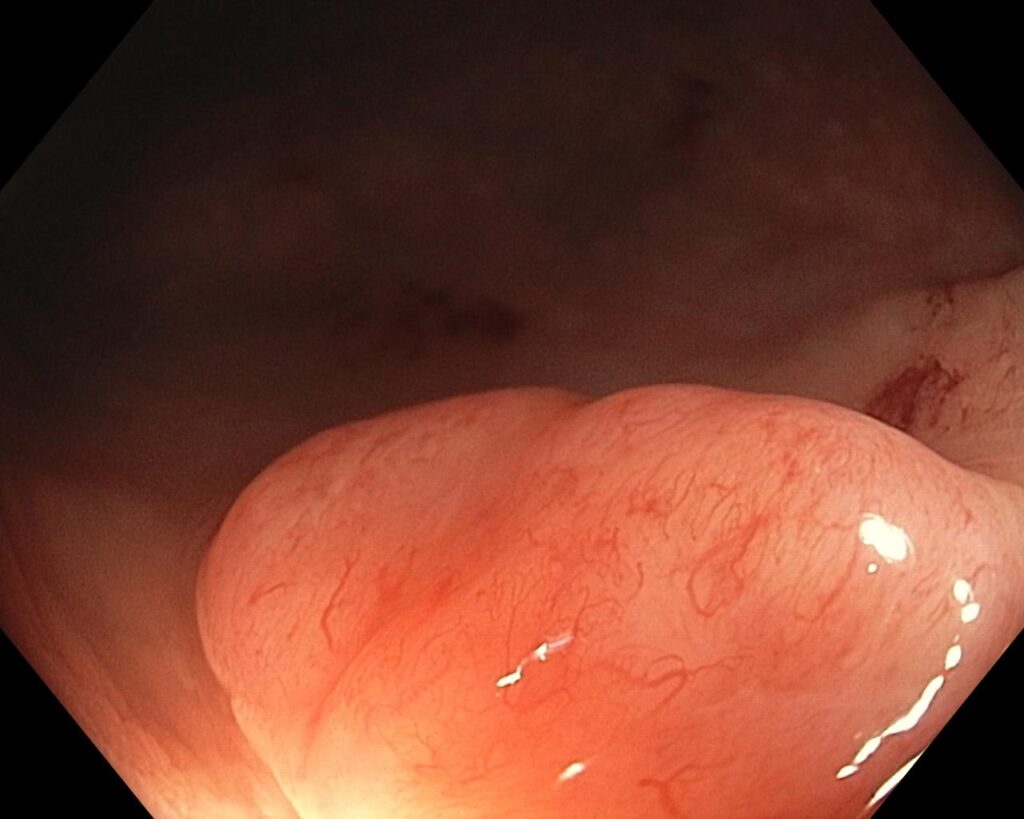
A 35-year-old woman with a family history of Crohn’s underwent colonoscopy for constipation and iron deficiency anemia. An incidental subepithelial lesion was found 1-2 cm from the anal verge. Endoscopic impression favored NET, but bite-on-bite biopsies came back as rectal tonsil.
The group was split. Several members noted elongated, stretched vessels typical of NETs, while another member annotated granular mucosa that could support rectal tonsil. One member recommended band EMR for a more complete specimen and noted that if the biopsy is correct, the patient should be tested for syphilis and HIV. When biopsy and endoscopic appearance disagree, complete resection gives the pathologist the best answer.
 1")
2. ERCP Cannulation Masterclass
A novice ERCPist asked whether to approach with the sphincterotome bowed with the papilla straight ahead, or from a 10-11 o’clock angle. The answer turned into one of the group’s best teaching threads. Key principles from one experienced member: “80% of your cannulation is proper positioning.” Wire-first, always.
Never advance the sphincterotome before confirming you are in the CBD. Minimal bow. Early precut: “5 minutes to cannulate, then precut.” Haraldsson Type 3 papilla is ideal for precut. On equipment: the DASH sphincterotome was preferred, DreamTome second, but “all is irrelevant if you can’t position yourself appropriately.” Cannulation is a positioning problem.
 2")
3. Complex Post-Sleeve Gastrectomy Fistula: Salvage Options
A patient with a persistent proximal staple-line leak/fistula after sleeve gastrectomy. The treatment history is exhaustive: multiple surgical revisions, repeated fully covered bariatric stents, VacStent therapy, repeated EsoSponge therapy, combined sponge-plus-stent approaches, APC conditioning, OTSC clip closure, and BARS closure attempts.
A chronic residual fistula tract persists. The presenting physician asked whether anyone has experience with autologous stromal vascular fraction or stem cell therapy injected into the fistula tract. No one responded with direct experience. The silence reflects how new this approach still is.
4. Upadacitinib Complication: PE/DVT in Bedridden Crohn’s Patient
A patient with extensive ileocolonic fistulating Crohn’s, unable to afford biologics, was started on upadacitinib. He then fell, developed a back hematoma that got infected and was drained, became bedridden, and developed PE/DVT. No anticoagulation had been given during the bedridden period.
One member identified the gap immediately: prophylactic anticoagulation should have been given while bedridden, regardless of the JAK inhibitor. Another member shared his practice of starting apixaban 2.5mg BD for one month in patients with severe IBD flares while waiting for advanced therapy to take effect. JAK inhibitors carry a class-wide thrombotic risk signal. VTE prophylaxis should be considered proactively.
 3")
5. Oropharyngeal Ulceration: Beyond the GI Tract
A 50-year-old male with odynophagia. EGD found ulcerated lesions at the tongue base, epiglottis, and aryepiglottic folds. Esophagus, stomach, and duodenum were completely normal. One member suggested relapsing polychondritis.
Another broadened the differential: Behcet’s, vitamin deficiency (B12, folate), viral causes (CMV, herpes, HIV), and NSAID-induced ulceration. Both agreed on rheumatology referral. Isolated oropharyngeal/laryngeal ulceration with a normal GI tract below the UES should prompt consideration of systemic inflammatory conditions, infections, and drug effects.
 4")
Quick Cases
March 11
- Tofacitinib patient follow-up from Issue 1. Enteroscopy showed patchy villous atrophy and possible lymphangiectasias in the jejunum with aphthous ulcers. One member identified villous atrophy. Another suggested checking coeliac serology. No granuloma on histology, only focal active colitis with cryptitis and architectural distortion.
March 14
- Rectal polyp EMR follow-up from Issue 1. CT showed an 11mm internal iliac lymph node. Reassurance given: no submucosal invasion on pathology, reactive node, not concerning.
- Endoscopic fecaloma treatment. Case reports of coca-cola injection via colonoscopy noted.
March 15
- Hemorrhoidal banding with variceal band ligator. Images and video shared. EBL is only for internal hemorrhoids above the dentate line. Banding below the dentate line is painful.
March 19
- Endoscopic fecaloma treatment (again). Two separate members asked about this within a week. The repeated interest suggests a practical gap worth covering.
March 7
- EUS-guided choledochoduodenostomy and Hot Axios article request. A 13-page GIE paper was provided same day.
Resource Sharing
Three major pancreatico-biliary textbooks shared in one evening: Endoscopic Ultrasound Management of Pancreatic Lesions, Advanced Therapeutic Endoscopy for Pancreatico-Biliary Diseases, and Updates in Pancreatic Endotherapy. ESsCD 2025 Updated Guidelines on Coeliac Disease shared. Two-part YouTube talk on ERCP cannulation tips and tricks shared.
Community Notes
- One senior member continued circling back to unresolved cases from Issue 1, asking for histopathology updates. This longitudinal tracking is one of the group’s strongest features.
- DeepSeek appeared again in clinical discussions. The group continues to treat AI-generated differentials as a starting point, not a conclusion.
- Several new members joined via the group link during this period.
What’s Next
- Master GI Bleeding Management — “The Ultimate Guide to GI Bleeding”
- Join EndoCollab — Access our full case library, expert discussions, and continuing education.
