
COMMUNITY DIGEST
3 featured cases and 5 quick consultations from the EndoCollab WhatsApp community between May 25 – June 7, 2026. Three featured cases from the WhatsApp group this period: a 19-year-old with ileocecal ulcers caught between Crohn's disease and intestinal tuberculosis (with a dramatic clinical update), a young heavy lifter with rectal ischemic injury raising the question of SRUS, and an achalasia food impaction that sparked a pharmacology discussion on LES relaxation.
In this issue
- Crohn's Disease vs. Intestinal Tuberculosis: When Negative Tests Do Not Rule Out TB
- Solitary Rectal Ulcer Syndrome in a Young Heavy Lifter
- Achalasia Food Impaction: Can Propofol Relax the Lower Esophageal Sphincter?
- Quick cases: Black Discoloration of the Distal Esophagus: Melanosis vs. Melanoma; Eosinophilic Esophagitis with a Suspicious GEJ Lesion; Complex Crohn's Disease: Biologic Failure, Abscess, and Surgical Timing; Acid Ingestion: Endoscopy Timing, NG Tube Placement, and Zargar Grading; Afferent Loop Stricture with Pneumobilia After Billroth II Gastrectomy
Featured Cases
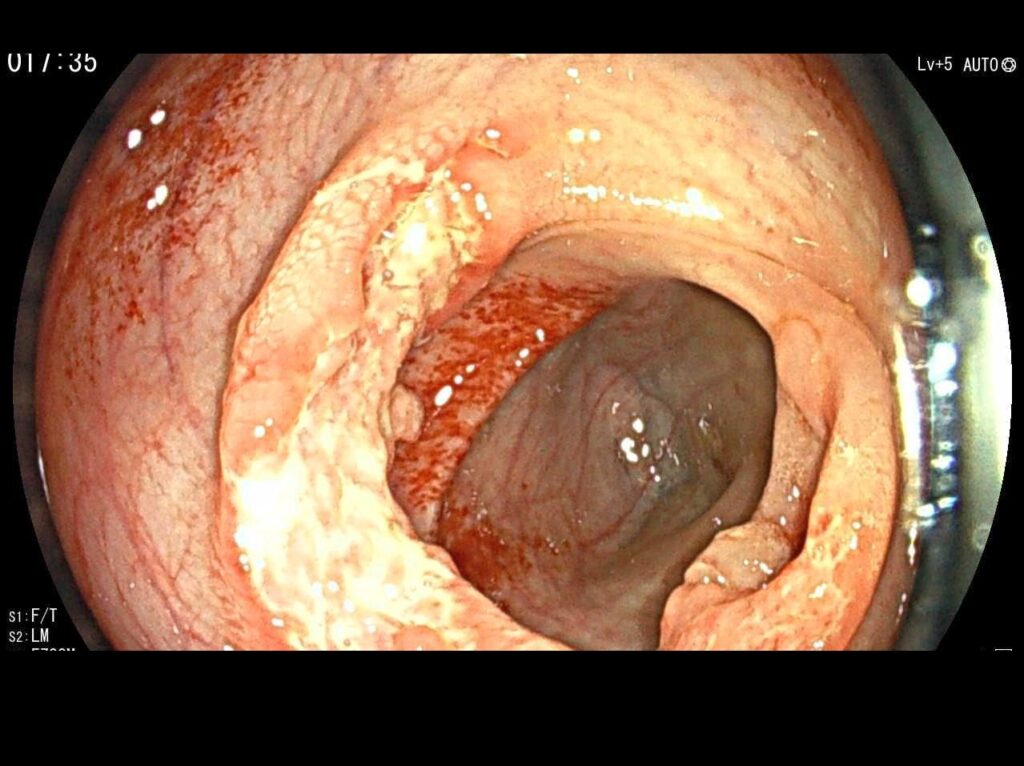
1. Crohn's Disease vs. Intestinal Tuberculosis: When Negative Tests Do Not Rule Out TB


A 19-year-old female from a TB-endemic region presented with three months of bloody diarrhea, significant weight loss, iron deficiency anemia, intermittent low-grade fever, and a history of TB contact. Colonoscopy showed predominant ileocecal involvement with a markedly inflamed, distorted ileocecal valve, a large transverse ulcer involving the valve and opposing fold, and additional deep ulcers in the terminal ileum and ascending colon with intervening normal mucosa.
CT enterography demonstrated terminal ileal and ileocecal wall thickening with multiple mesenteric lymph nodes showing central necrosis. Scattered centrilobular pulmonary nodules were also noted. Despite these red flags, preliminary histopathology favored Crohn's disease: architectural distortion, focal cryptitis, and granulation tissue, but no granulomas. AFB stain was negative, TB PCR was negative, and TB culture remained pending.
The community consensus leaned strongly toward TB. Key reasoning: (1) the transverse ulcer pattern favors TB over the longitudinal ulcers more typical of Crohn's, (2) necrotic mesenteric lymph nodes are a strong indicator of TB, (3) the pulmonary nodules and TB contact history add significant pre-test probability. Members recommended Quantiferon testing, ID and pulmonology consultation, empiric anti-TB therapy, and withholding immunosuppressive therapy until TB could be more confidently excluded. Starting immunosuppressants in a patient with undiagnosed TB risks disseminated disease.
The case took a sobering turn two days later. The patient developed headache, photophobia, behavioral changes, encephalopathy, and a generalized tonic-clonic seizure. MRI brain showed left perisylvian frontotemporal cerebritis with leptomeningeal enhancement. CSF analysis revealed markedly elevated protein (1306) and low glucose (1.99). The clinical picture became consistent with disseminated TB with CNS involvement, and the patient was started on empiric anti-TB therapy along with dexamethasone, broad-spectrum antibiotics, and antiepileptic treatment.
Clinical Pearl: When clinical and radiological features strongly suggest intestinal TB (necrotic lymph nodes, transverse ulcers, pulmonary nodules, TB contact), empiric anti-TB therapy is warranted even when histology, AFB stain, and PCR are negative. Starting immunosuppression before excluding TB can lead to disseminated disease, including CNS involvement. ATT for intestinal TB should be given for at least one year, not the standard six-month regimen.
2. Solitary Rectal Ulcer Syndrome in a Young Heavy Lifter
A 40-year-old male presented with rectal pain and bleeding. He was a heavy lifter who drove for work. He had a history of hemorrhoids, but no clear constipation. He actually reported 3-4 peanut butter-consistency stools daily with incomplete evacuation. A surgeon found grade 4 hemorrhoids on exam. Intraoperative colonoscopy revealed a lesion with biopsy showing features of ischemic-type injury.
The initial differential centered on SRUS versus rectal prolapse. One member pointed out that true ischemic injury should not occur in the rectum of a young patient because rectal blood supply is dual systemic. The ischemic histology pattern, combined with the clinical history, pointed toward mucosal prolapse syndrome or SRUS rather than a primary vascular event.
Discussion then turned to the mechanism. Heavy lifting with valsalva is associated with prolapse of hemorrhoids and potentially rectal prolapse, but typically requires pre-existing pelvic floor weakness. Marathon runners are well-established to develop ischemic colitis and rectal changes, but the association with heavy lifters is less documented. One member suspected dyssynergic defecation as the underlying problem. Recommendations included anorectal manometry, balloon expulsion testing, and consideration of MR defecography to evaluate for occult prolapse.
A senior member noted that SRUS biopsies typically show significant thickening of the muscularis mucosa that obliterates the lamina propria, and that taking biopsies from SRUS tissue often feels like grating on a rock with the forceps.
Clinical Pearl: In a young patient with rectal ischemic-type histology, consider SRUS and mucosal prolapse syndrome. The rectum has dual systemic blood supply, so true ischemia here should prompt a search for mechanical causes. Anorectal manometry, balloon expulsion testing, and MR defecography help refine the diagnosis. Ask pathology to stain for muscle fibers if SRUS is in the differential.
3. Achalasia Food Impaction: Can Propofol Relax the Lower Esophageal Sphincter?
A patient with severe achalasia presented with food impaction. The endoscopist attempted removal under conscious sedation with midazolam (1 mg) and fentanyl (25 mcg), but the esophagus was packed with food particles that could not be cleared. The intensive care team was called to intubate the patient and secure the airway using a rapid sequence intubation protocol.
After intubation with propofol (100 mg), rocuronium (100 mg), and fentanyl (50 mcg), a second endoscopy was performed. The food was gone and the endoscope passed without difficulty. The presenting endoscopist asked whether the medications could have relaxed the esophageal sphincter.
The pharmacology discussion was focused. Rocuronium is a non-depolarizing neuromuscular blocker that targets nicotinic receptors at the skeletal muscle motor endplate. The LES is smooth muscle and does not express nicotinic receptors, so rocuronium should not affect it. The group then considered propofol, which has known smooth muscle relaxing properties and is the more plausible candidate for LES relaxation. Glycopyrrolate and atropine, both anticholinergics sometimes used in RSI protocols, could also contribute to sphincter relaxation by blocking muscarinic tone.
One member pointed out that some anesthesiologists routinely use glycopyrrolate to reduce secretions during intubation. In this case, the presenting endoscopist confirmed the protocol included only propofol, rocuronium, and fentanyl, with no anticholinergics. The consensus was that propofol was the most likely explanation for the observed LES relaxation.
Clinical Pearl: Rocuronium targets skeletal muscle nicotinic receptors and should not relax smooth muscle structures like the LES. Propofol has smooth muscle relaxing properties and is the more likely cause of LES relaxation in this setting. Anticholinergics used in RSI protocols (glycopyrrolate, atropine) can also reduce LES tone. When encountering unexpected esophageal emptying after intubation in achalasia, review the full medication list before attributing the effect to a single agent.
Quick Consultations
Esophageal Pathology · Black Discoloration of the Distal Esophagus: Melanosis vs. Melanoma

A patient with two months of dyspepsia had upper endoscopy revealing black discoloration involving the distal esophagus. The community identified this as esophageal melanosis, a benign condition caused by melanocyte proliferation in the esophageal epithelium. The key differential is malignant melanoma, which should be excluded with biopsy. One member also raised the possibility of subtle submucosal hemorrhage from retching as an alternative explanation for focal dark discoloration.
EGD Findings · Eosinophilic Esophagitis with a Suspicious GEJ Lesion


A 44-year-old male with occasional reflux had esophageal trachealization consistent with eosinophilic esophagitis and a lesion just below the esophagogastric junction. The question was whether this represented intestinal metaplasia. The community noted that the distal lesion was more likely reactive foveolar hyperplasia from reflux injury, given the clear erosive esophagitis and hiatus hernia visible on the images. Intestinal metaplasia at the GE junction is unlikely outside of advanced atrophic autoimmune gastritis. Another member commented that the glands in the first 5 to 10 mm of the stomach resemble antral-type glands, and inflammation of these cardial glands (carditis) can mimic metaplasia endoscopically.
IBD Management · Complex Crohn's Disease: Biologic Failure, Abscess, and Surgical Timing
A 29-year-old malnourished male (BMI 16) with small bowel Crohn's, a pelvic abscess with enteroenteric fistula, and biologic experience (anti-TNF, ustekinumab, vedolizumab) was readmitted with pain on antibiotics. The abscess was too small and too intermixed with bowel for percutaneous drainage. The community identified five predictors of treatment failure: very early onset IBD, fistulizing phenotype, male gender, biologic experience with prior failures, and need for surgery. Vedolizumab was likely primed to fail in this setting based on the LOVE-CD trial data. Recommendations included exclusive enteral nutrition (EEN) over TPN, consideration of infliximab at 10 mg/kg every 4 weeks with therapeutic drug monitoring, and referral to a high-volume IBD center. Corticosteroids were contraindicated given the abscess and likely surgical need. The group agreed that surgery appeared inevitable, and that an MDT setup was needed to avoid conflicting recommendations.
Caustic Ingestion · Acid Ingestion: Endoscopy Timing, NG Tube Placement, and Zargar Grading
A patient ingested muriatic acid. CT showed no perforation. Endoscopy at two hours post-ingestion showed Zargar IIA esophageal injury and Zargar IIIB gastric necrosis. The community debated NG tube placement. Arguments against: NG tubes increase pharyngeal irritation and may not be tolerated, and in the setting of significant gastric necrosis, a nasojejunal (NJ) tube for feeding is preferred. Arguments for: gastric outlet obstruction without drainage is dangerous, and tubes do not cause perforations, ischemia does. The consensus on timing: endoscopy is safe within 48 hours provided there is no perforation, should be avoided between days 5 and 15 (highest perforation risk), and is safe again after 3 weeks. CT with gastrografin is recommended before endoscopy if perforation is suspected.
Post-Surgical Endoscopy · Afferent Loop Stricture with Pneumobilia After Billroth II Gastrectomy
A 76-year-old man who had distal gastrectomy with Billroth II reconstruction in 2008 for gastric carcinoma presented with vomiting and reflux triggered by larger meals. Endoscopy showed the afferent limb was strictured and the scope could not pass. CT revealed significant pneumobilia without clinical cholangitis. The stricture appeared very focal, and the community recommended CRE balloon dilation as the first-line approach rather than revision surgery, which would be a major undertaking more than 15 years post-resection. The pneumobilia raised questions about bilioenteric communication. One member proposed that a blind afferent loop with partial stricturing and SIBO could generate gas that creates back-pressure on the sphincter of Oddi, leading to incompetence.
What’s Next
Every case in this digest came from real conversations in the EndoCollab private WhatsApp community, 650+ practicing endoscopists discussing cases daily from every continent. Lifetime members get permanent access to the group, plus the full EndoCollab case library of 1,700+ teaching cases, technique videos, and references.
