
COMMUNITY DIGEST
4 featured cases and 6 quick consultations from the EndoCollab WhatsApp community between June 8 – July 17, 2026. Four featured cases from the WhatsApp group this catch-up window: recurrent small-bowel obstruction that looked like IBD at laparotomy without a resectable stricture, multiple antro-pyloric openings from malignant fistulation in metastatic pancreatic cancer, a descending-colon tumor missed behind a poor prep, and a cecal lesion where the non-lifting sign correctly steered care to surgery.
In this issue
- Jejunal Crohn's Behind Recurrent Small-Bowel Obstruction
- Multiple Antro-Pyloric Openings from Malignant Fistulation
- The Descending-Colon Cancer Hidden by a Poor Prep
- Respect the Non-Lifting Sign at the Cecal/Appendiceal Ostium
- Quick cases: Enterobius vs Whipworm at Colonoscopy; Cervical Esophageal Inlet Patch; Small Esophageal Leiomyoma; Acute Bloody Diarrhoea: Resist Scoping Too Early; Soft Colonic Submucosal Lesion and the Pillow Sign; Radiolucent Foreign-Body Ingestion with a Negative X-ray
Featured Cases
1. Jejunal Crohn's Behind Recurrent Small-Bowel Obstruction


A 53-year-old man presented after about 1.5 years of recurrent subacute intestinal obstruction managed conservatively. He reported chronic bloating without vomiting and had no prior abdominal surgery. An outside OGD was reported as normal. Serial erect abdominal films from March through June 2026 showed persistent dilated small-bowel loops with air-fluid levels. An older CT and a subsequent MR enterography showed jejunal mural thickening, pre-stenotic chronic dilatation, mesenteric panniculitis, and lymphadenopathy. Faecal calprotectin was 569 to 592. Ileoscopy showed only two aphthous ulcers. Volumen contrast for MRE transiently precipitated an obstructive episode.
At exploratory laparotomy the surgeon found creeping fat and dilated small bowel, but after running the bowel from Treitz to the ileocecal valve found no discrete stricture, block, or fistula. Imaging and operative findings therefore disagreed on whether a fixed mechanical transition point was present.
The community leaned strongly toward upper-GI/jejunal Crohn's. Key points: put the whole picture together (chronic symptoms, elevated calprotectin, aphthous ulcers, creeping fat, imaging) rather than waiting for one confirmatory test; upper-GI Crohn's is often an aggressive phenotype favoring anti-TNF with a thiopurine; and the next diagnostic step should be chosen by how far the disease sits from the ileocecal valve (capsule for mapping if no stricture is confirmed; balloon-assisted enteroscopy if the target looks reachable and histology is needed). Empiric IBD therapy with interval imaging was also considered an acceptable option after shared decision-making.
Clinical Pearl: Upper-GI/jejunal Crohn's can present as recurrent SBO with creeping fat but no resectable stricture at laparotomy. Synthesize the clinical, laboratory, endoscopic, imaging, and operative clues, then choose capsule versus balloon enteroscopy based on distance from the ileocecal valve rather than waiting for a single confirmatory test.
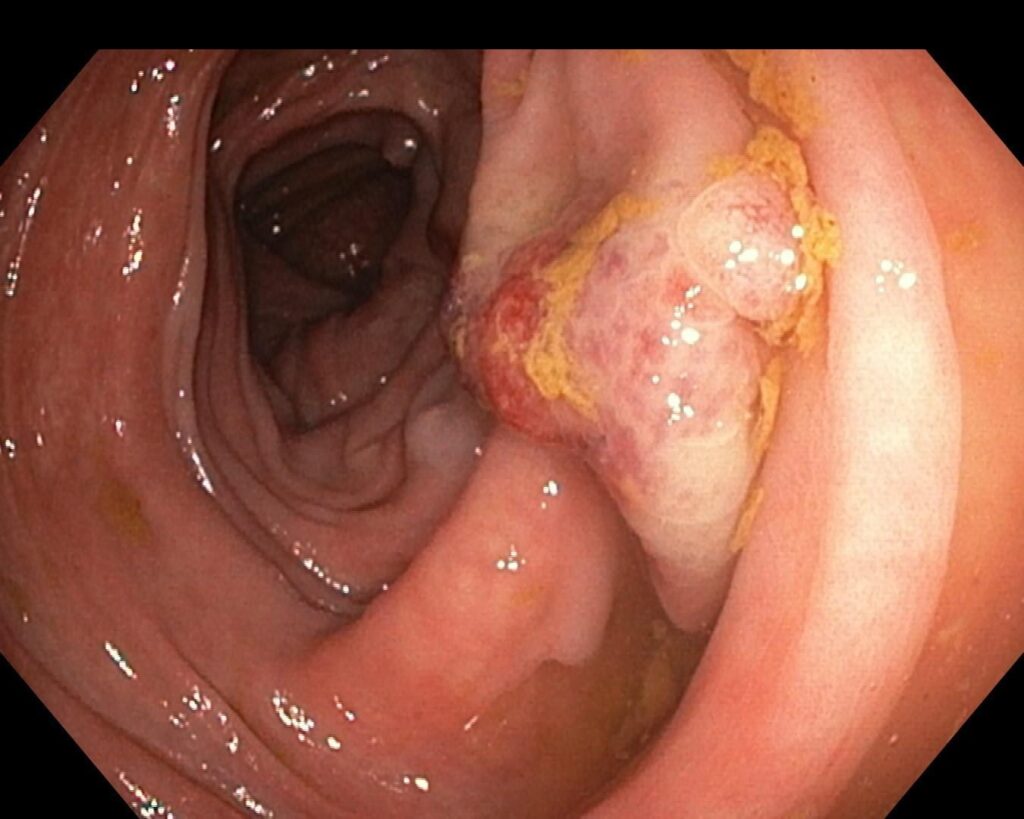
2. Multiple Antro-Pyloric Openings from Malignant Fistulation


A 60-year-old with metastatic pancreatic ductal adenocarcinoma, cirrhosis, and portal hypertension presented with hematemesis. Endoscopy of the antro-pyloric region showed multiple openings (one true pylorus plus additional openings) and an ulcerated, tightly stricturing growth in the duodenal bulb that the scope could not traverse.
The community read the appearance as malignant fistulation, possibly with prior palliative radiation contributing, and predicted that adjacent fistulous openings would coalesce over time. No vessel amenable to endoscopic hemostasis was identified, and the patient was still eating. Management stayed within a palliative frame: characterise the ulcerated stricture, look carefully for a treatable bleeding vessel, and avoid over-interpreting the extra openings as anatomic variants.
Clinical Pearl: Multiple antro-pyloric openings in locally advanced upper-GI or pancreatic malignancy should raise malignant fistulation (or post-radiation change). Characterise the ulcerated stricture, search for a treatable bleeding vessel, and keep decisions inside the palliative context.
3. The Descending-Colon Cancer Hidden by a Poor Prep


A 56-year-old man had CT showing thickened/stenosing descending and sigmoid colon, thickened terminal ileum and jejunal loops, and a distended transverse colon (7 cm). Initial suspicion was IBD. The first colonoscopy was aborted at mid-sigmoid because of feces. Distal sigmoid lesions raised a differential of ischemic colitis, severe SCAD, inflammatory pseudopolyps versus pedunculated polyps, and inverted diverticulum. Biopsy initially suggested SCAD/ischemic colitis.
On repeat colonoscopy with adequate prep, a tumor was found in the descending colon upstream of the previously seen lesions. That segment had not been reached on the first exam because of poor preparation. Severe sigmoid diverticulosis had also made proximal progress difficult.
Clinical Pearl: Do not anchor on SCAD or inflammatory polyps after an incomplete, poorly prepped exam. An unreached segment can conceal colorectal cancer. Complete or promptly repeat the colonoscopy before settling the diagnosis.
4. Respect the Non-Lifting Sign at the Cecal/Appendiceal Ostium
A 44-year-old with no personal or family history had a lesion at the cecal/appendiceal ostium previously discussed for endoscopic resection (cap-assisted or underwater EMR, and even EFTR). A non-lifting sign prompted referral for right hemicolectomy instead.
Final histology showed G2 (focally mucinous) adenocarcinoma at the cecal/appendiceal ostium invading full-thickness muscularis (pT2), with serrated areas showing high-grade dysplasia; an appendiceal serrated adenoma with intramucosal carcinoma (pT1); 12 nodes negative (pN0); and clear margins. Consensus was that even if EFTR had been attempted, hemicolectomy would still have been required. The non-lifting sign steered the correct decision.
Clinical Pearl: A non-lifting sign on a cecal/appendiceal-ostium lesion is a red flag for deep invasion. Favour surgical referral over heroic endoscopic resection at a site where EMR/EFTR would not have been curative anyway.
Quick Consultations
Enterobius vs Whipworm at Colonoscopy
Incidental small worms were seen on follow-up ileocolonoscopy after completed ATT for abdominal TB. The group favoured Enterobius vermicularis (short worms, right colon/appendiceal region) over Trichuris. Grab a worm for microscopy if unsure, but mebendazole or albendazole covers both.
Cervical Esophageal Inlet Patch


An incidental salmon-colored patch in the proximal esophagus with mild pill-related discomfort only. Consensus: inlet patch, PPI, rarely malignant. Characterise with a distal cap and NBI before considering treatment.
Small Esophageal Leiomyoma

Incidental subepithelial lesion under about 2 cm with only mild reflux symptoms. If the diagnosis is secure and GIST is excluded (CKIT), surveillance at roughly 2-year intervals is reasonable.
Acute Bloody Diarrhoea: Resist Scoping Too Early
A 40-year-old with three days of bloody diarrhoea, RLQ pain, WBC 23k, and CRP 165. Wide infectious and inflammatory differential. Early colonoscopy (and even early calprotectin) often starts a wild-goose chase. Treat the acute illness, then reassess.
Soft Colonic Submucosal Lesion and the Pillow Sign
A soft ~40 cm lesion with a positive pillow sign raised hematoma, duplication cyst, inverted diverticulum, and lipoma. Superficial biopsies were unhelpful. Image with CT (too high for EUS) and avoid deep biopsy if inverted diverticulum remains plausible.
Radiolucent Foreign-Body Ingestion with a Negative X-ray
Suicidal ingestion of a beaded bracelet with abdominal pain and a negative plain film. Plastic beads may be invisible on X-ray and even CT. Escalate imaging (US/CT/C-arm) and base urgency on symptoms and object type.
Community Notes
- Underwater polypectomy: you do not have to switch off insufflation. Simplest is not to touch the air/CO2 button during the resection.
- Chromoendoscopy in G6PD deficiency: avoid methylene blue; use indigo carmine or virtual chromoendoscopy/NBI.
- Cola for phytobezoar or diverticular fecalith: for volumes over about 500 mL, shake first to remove carbonation. Bubbles hinder the mobilising effect.
- Uncovered duodenal stents embed within weeks. Plan removal within about 3 weeks, or use APC / stent-in-stent strategies with surgical backup if already embedded.
- Migrated malignant hilar stent: prefer a longer straight stent so adequate length sits beyond the stricture rather than a pigtail that wastes length in the curl.
Join the conversation. These cases come from EndoCollab’s private WhatsApp community. Lifetime members get permanent access to the group and the full case library.
