
Argon plasma coagulation (APC) ranks among the most frequently performed therapeutic interventions in gastrointestinal endoscopy. While APC serves multiple purposes beyond hemostasis, mastering the nuances of bleeding control: whether for prophylaxis or active treatment: remains fundamental to our practice. Today, I’ll share four refined techniques that can significantly improve your outcomes when treating angiodysplasias, GAVE, and radiation proctitis.
The Foundation: Understanding APC Applications
APC proves invaluable for treating various bleeding lesions throughout the GI tract. The key lies not just in knowing when to use it, but how to apply it effectively. These four techniques represent years of refinement in my practice, each suited to specific clinical scenarios.
Technique 1: The Short Burst Method
This represents the classic, conservative approach that most of us learned initially. The technique involves advancing the catheter distally beyond the endoscope tip, positioning close to the target lesion, and applying brief, controlled bursts of energy.
The short burst method works as a “target and shoot” technique. You maintain a short distance to the target and deliver energy in discrete pulses. This conservative approach minimizes thermal injury while providing adequate coagulation for most superficial lesions.
I frequently use this method for gastric AVMs and small bowel angiodysplasias. The controlled energy delivery reduces perforation risk while achieving effective hemostasis in straightforward cases.
Continue reading with a membership
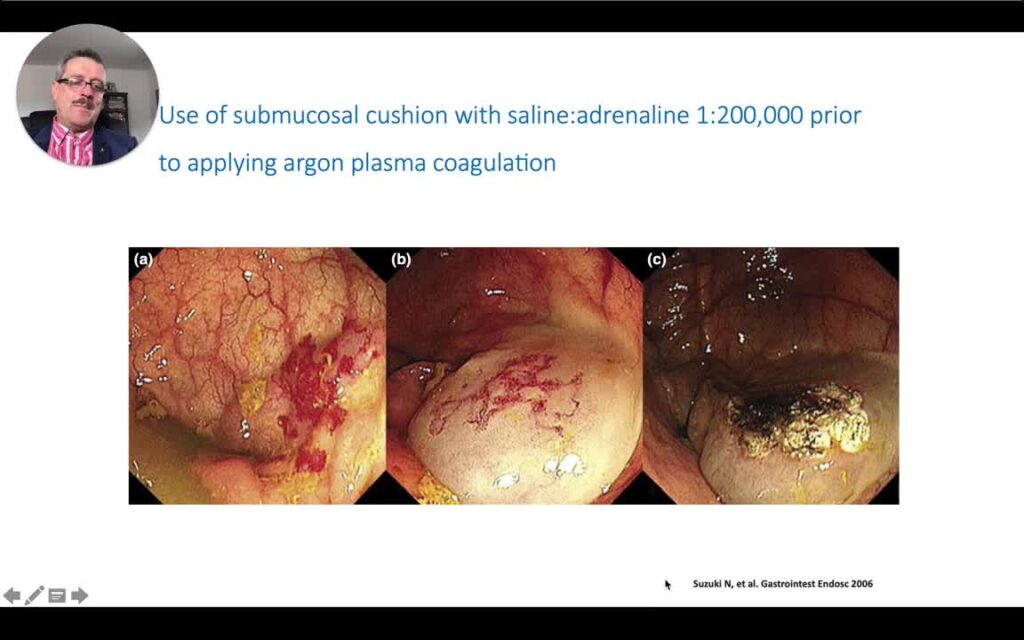
Learn advanced APC techniques including the long burst strategy for GAVE and radiation proctitis, plus the submucosal cushion safety method for large angiodysplasias. Master the clip-after-burst technique for anticoagulated patients to significantly reduce rebleeding risk.
Plus full video with chapters and English captions.
Already a member? Log in
