
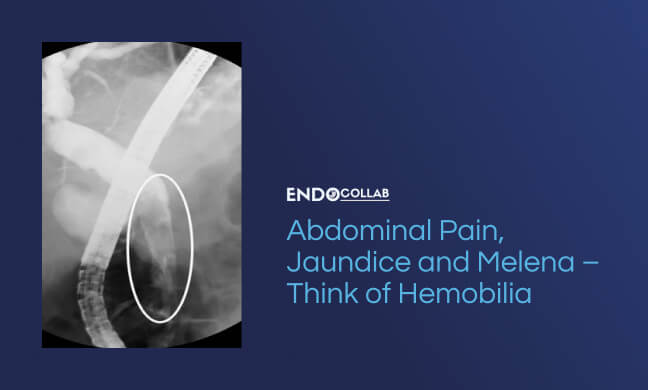
A 58-year-old patient with NAFLD, diabetes mellitus and hypertension underwent a liver biopsy for a 3 cm nodule in segment VI of the liver. About 24-hours later the patient complained of acute onset abdominal pain, followed by jaundice and chills. He also had melenic stools. On arrival to the emergency room his blood pressure was 100/50 and the heart rate was 100 ppm. The sclerae were icteric. There was right upper quadrant abdominal pain. CT of the abdomen showed dilated bile duct with possible common bile duct sludge or stones. The ERCP image is shown.

Emergent ERCP demonstrated of multiple irregular filling defects within the proximal and distal biliary tree. The common bile duct was dilated to about 18 mm. A biliary sphincterotomy was performed and multiple blood clots were extracted with a balloon. A 10Fr 10 cm plastic stent was inserted. His symptoms improved rapidly, the bilirubin started to trend down and the bile duct stent was removed after 4 weeks.
Additional Case:

Discussion:
Hemobilia results from injury to the biliary tree which may arise from primary cancer, tumor invasion trauma, gallstones, liver biopsy, radiofrequency embolization, trans-arterial chemo-ablation (TACE) for liver tumors, pseudoaneurysmss, and rarely vasculitides and is often serious and life threatening. The most common artery involved appears to be right hepatic artery.1 It generally presents as epigastric pain, icterus and GI bleed 2, commonly called the Quinke’s triad, however only 22% of the patients have all three features. Depending upon the underlying cause, bleeding generally presents days to months after the initial injury. Especially when jaundice is absent, and only abdominal pain and GI bleeding are present, an EGD is performed first. Unfortunately, hemobilia is often missed, as the papilla is not closely observed during EGD or the bleeding may be intermittent. Thus, we highly recommend performing EGD with distal transparent cap to properly inspect the papilla, or directly use a side viewing duodenoscope.
A CT of the abdomen is also useful in the work-up of suspected hemobilia, as it will show blood clots or ‘periportal tracking’, especially in the patients with abdominal trauma, and also rule out any tumors or paseudoaneurysms. ERCP with cholangiography may show filling defects in the biliary tree. The treatment is quadruple: a) decompressing the biliary tree, b) providing adequate drainage, c) transfuse blood and correct coagulopathy, if necessary, and d) treating the underlying or precipitating condition.
Further reading:
1. Tessier DJ, Fowl RJ, Stone WM, et al. Iatrogenic hepatic artery pseudoaneurysms: an uncommon complication after hepatic, biliary, and pancreatic procedures. Ann Vasc Surg 2003;17(6):663-9.
2. Quinke H. Ein Fall von aneurysma der leberarterie. Klin Wochenschr 1871; 8: 349-51
3. Walter JF, Paaso BT, Cannon WB. Successful transcatheter embolic control of massive hematobilia secondary to liver biopsy. Am J Roentgenol 1976; 127: 847-9
Hemobilia. AWhat Are the Main Causes of Hemobilia?ERCP – Hemobilia After Transhepatic Arterial Chemoembolization (TACE)CT Scan Unveils Cirrhosis, HCC, and Portal Vein Thrombosis: A Comprehensive Look at Hemobilia and Portal Hypertensive Biliopathy

30 Responses
1
1GmZyaJMY
1*1
1*if(now()=sysdate(),sleep(15),0)
10″XOR(1*if(now()=sysdate(),sleep(15),0))XOR”Z
1-1; waitfor delay ‘0:0:15’ —
1-1); waitfor delay ‘0:0:15’ —
1-1 waitfor delay ‘0:0:15’ —
1yiCoxbNk’; waitfor delay ‘0:0:15’ —
1-1)) OR 320=(SELECT 320 FROM PG_SLEEP(15))–
1i2L23B0H’) OR 431=(SELECT 431 FROM PG_SLEEP(15))–
1*DBMS_PIPE.RECEIVE_MESSAGE(CHR(99)||CHR(99)||CHR(99),15)
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1