
Case Report & Technique
A systematic, image-guided approach to hot-snare R0 resection of a 12 mm granular LST in the ascending colon — featuring the suction-mark trick, interventional chromoendoscopy with Eleview®, and prophylactic clipping.
Diana Dougherty, MD
Department of Gastroenterology, Carilion Memorial Hospital, Virginia Tech Carilion School of Medicine, Roanoke, USA
Klaus Mönkemüller, MD, PhD, FASGE, FJGES
Department of Gastroenterology, Carilion Memorial Hospital, Virginia Tech Carilion School of Medicine, Roanoke, USA
Published: February 2026 | EndoCollab
Abstract
We present a step-by-step endoscopic resection of a 12 mm granular laterally spreading tumor (LST-G) in the ascending colon using interventional chromoendoscopy and hot-snare EMR. Key techniques discussed include the suction-mark trick for polyp relocalization, submucosal lifting with Eleview® to achieve an oncologic R0 margin, sizing with the Captivator™ 15 mm snare, and prophylactic clipping tailored to individual patient risk factors for post-polypectomy bleeding.
Keywords: laterally spreading tumor, LST-G, ascending colon, hot snare EMR, interventional chromoendoscopy, Eleview, R0 resection, suction-mark trick, prophylactic clipping, colon polyp
⭐ Key Clinical Takeaways
- Any flat colonic lesion ≥10 mm qualifies as an LST; initial assessment should include location, morphology (granular vs. non-granular), and surface pattern (Kudo classification).
- The suction-mark trick — briefly suctioning mucosa adjacent to the polyp — creates a visible red submucosal mark that helps relocalize the lesion in a moving or debris-laden colon.
- Interventional chromoendoscopy with blue-dye submucosal injection (e.g., Eleview®, saline + indigo carmine) raises the lesion and demarcates neoplastic from normal tissue, facilitating R0 resection.
- Using the snare to measure lesion size before entrapment (Captivator™ 15 mm braided snare) allows confirmation that the polyp is fully within snare diameter.
- Hot snare EMR with electrosurgical current produces burned lateral and basal margins, reducing residual adenoma — an advantage over cold snare for LSTs.
- Prophylactic clipping should be individualized: right-sided location + hypertension + distance from home/emergency services = strong indication for clips even in outpatient settings.
Initial Assessment: Four Steps Before Resection
A flat polypoid lesion was identified in the ascending colon. Because it measured >10 mm, it met the definition of a laterally spreading tumor (LST). Before any resection is planned, four key steps are essential:
- Determine location — here, the lesion sits between two folds, creating a technical challenge for snare passage.
- Classify morphology — this is an LST-G (granular subtype), which carries lower submucosal invasion risk than LST-NG.
- Analyze surface pattern — high-definition WL and NBI show a regular cerebroid Kudo IIIL pit pattern with uniform vessels, consistent with low-grade dysplasia.
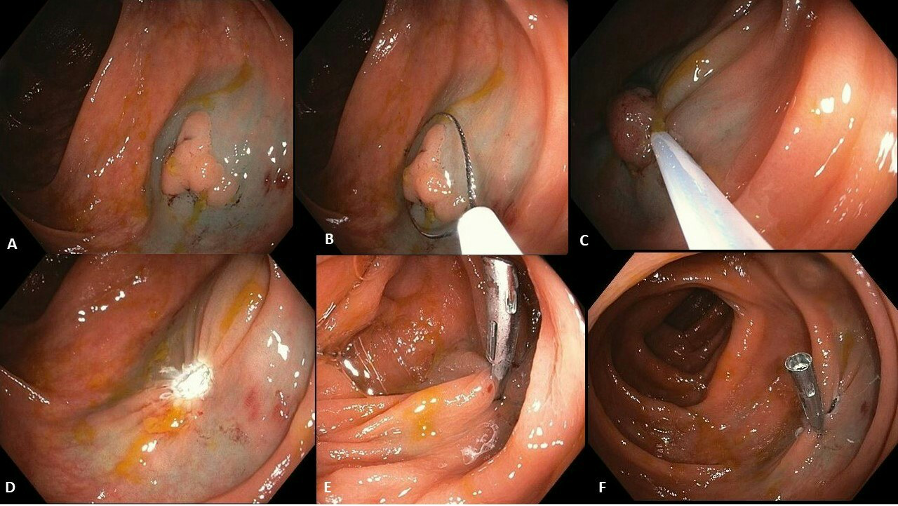
- Don’t lose the polyp — the suction-mark trick is applied at this stage (see below).
The Suction-Mark Trick
With the scope focused on the lesion, the endoscopist advances toward it and briefly suctions adjacent normal mucosa. This creates a red submucosal suction mark immediately next to the polyp. The mark persists for several minutes, serving as a beacon to relocalize the lesion after scope repositioning — especially valuable in: (1) patients whose colon moves significantly, (2) settings with residual debris, and (3) polyps in difficult anatomical locations.
Submucosal Injection and Interventional Chromoendoscopy
The LST was lifted using Eleview® (Cosmo Technologies, Ireland/Germany), though alternatives include normal saline + indigo carmine, methylene blue, or hydroxymethylcellulose solutions (e.g., Blue Eye). Two critical observations after injection:
- The lesion lifts uniformly, confirming no submucosal fibrosis — a positive lifting sign.
- The blue dye stains predominantly normal mucosa, highlighting the neoplastic tissue by contrast — this is the principle of interventional chromoendoscopy: using colorings to guide therapeutic decisions toward oncologic R0 resection.
Hot Snare EMR: Sizing, Entrapment, and Resection
A Captivator™ 15 mm braided snare (Boston Scientific, USA) was deployed. The open snare served dual purposes:
- Size measurement — with the snare fully open at 15 mm, the LST measured approximately 12 mm (smaller than snare diameter, confirming en-bloc resection is feasible).
- Full entrapment — the submucosal cushion allows the entire LST to be encircled above the snare wire.
The snare was tightly closed — almost achieving cold-snare tension — before applying electrosurgical current. The resulting specimen showed an endoscopic R0 resection: burned lateral and basal margins with no residual tissue. This thermal effect is the primary advantage of hot snare over cold snare for LSTs, explaining the lower adenoma recurrence rates with the hot technique.
Prophylactic Clipping: A Personalized Decision
This patient had two risk factors for post-polypectomy bleeding: right-sided colon location and hypertension. Additionally, the procedure was outpatient and the patient travels from a significant distance. Prophylactic clips were placed. Technical tip: deflate the colon before clip placement — this keeps the resection site small and ensures optimal clip apposition. After clipping, re-insufflate briefly to confirm placement.
While guidelines may not mandate clipping in all right-sided polypectomies, personalized endoscopy — accounting for individual patient risk and social factors — should always take precedence.
Conflict of Interest: Diana Dougherty and Klaus Mönkemüller declare no conflicts of interest with any companies, utensils, or products mentioned in this article.
How to Cite
Dougherty D, Mönkemüller K. Endoscopic Resection of LST in Ascending Colon. EndoCollab. 2026. Available at: https://endocollab.com
