
CASE REPORT
Abstract
Background: Bleeding peptic ulcer with a visible vessel (Forrest IIa) carries a high risk of rebleeding and requires prompt endoscopic hemostasis. Multiple modalities are available, including injection, thermal, and mechanical therapies, each with distinct technical considerations and anatomical suitability.
Case Presentation: We report an 80-year-old man with melena in whom esophagogastroduodenoscopy (EGD) revealed a large anterior duodenal ulcer with a visible vessel. Hemostasis was achieved using a 7 Fr injection gold probe — a bipolar multipolar electrocoagulation (MPEC) device — combining submucosal epinephrine injection with contact electrocoagulation.
Conclusion: The injection gold probe is a safe and effective tool for endoscopic hemostasis in anteriorly located duodenal ulcers. Device selection should be guided by ulcer location, technical accessibility, and operator familiarity. Caution is warranted given the risk of thermal injury and perforation in the duodenum.
Keywords: duodenal ulcer bleeding; hemostasis; injection gold probe; multipolar electrocoagulation; MPEC; endoscopic hemostasis; non-variceal upper GI bleeding; visible vessel
★ Key Clinical Takeaways
- Ulcer location relative to the endoscope is a critical technical factor: anteriorly positioned duodenal ulcers are ideally suited for injection gold probe therapy, whereas posteriorly located ulcers may be technically inaccessible.
- Coaptive coagulation — pressing the probe firmly against the vessel to achieve compression before activating current — is fundamental to effective bipolar/MPEC hemostasis.
- The injection gold probe combines epinephrine injection and contact electrocoagulation in a single device, reducing procedure complexity while delivering combination therapy superior to either modality alone.
- Risk of perforation exists with thermal hemostasis probes in the duodenum; judicious wattage, contact time, and pressure are essential to avoid deep thermal injury.
Case Presentation
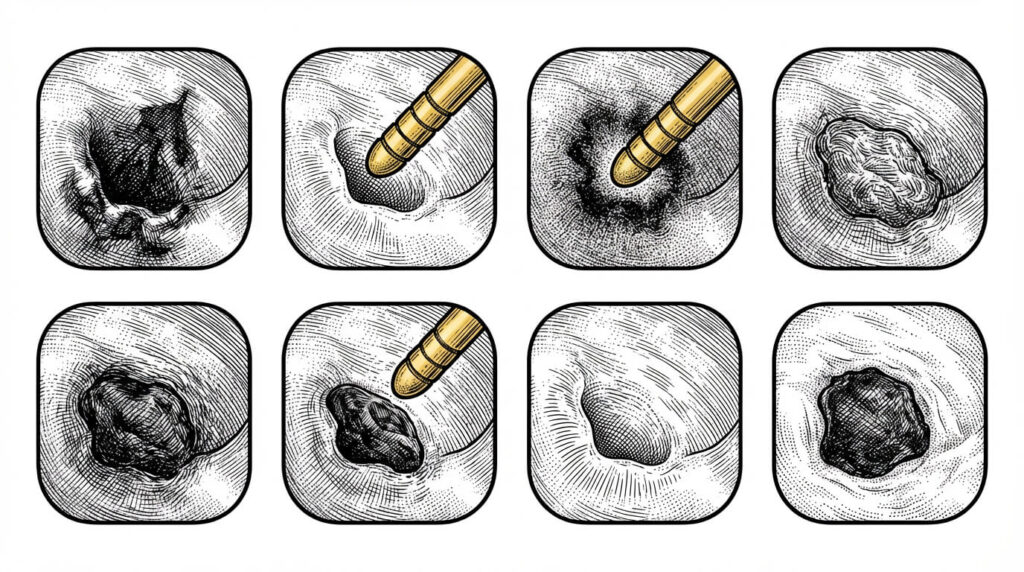
An 80-year-old man presented with melena. Esophagogastroduodenoscopy (EGD) revealed a large duodenal ulcer with a visible vessel, located anteriorly (Figure 1). Hemostasis was achieved with combination injection and contact electrocoagulation therapy using an injection gold probe.

Background: Endoscopic Hemostasis Methods
There is a large variety of tools available to achieve endoscopic hemostasis. These are broadly classified into injection, thermal, mechanical, and contact methods (1) (Figure 2).

Discussion
Device Description and Mechanism of Action
The injection gold probe catheter is a bipolar hemostasis device that combines injection capability with electrocoagulation to arrest bleeding. A mixture of saline and epinephrine is typically injected around the target area (e.g., visible vessel), followed by electrocauterization of tissue. The probe’s tip heats tissue using electrical current, coagulating tissue and blood to achieve hemostasis. The rounded tip provides a uniform burn and coagulation footprint, and the probe’s design reduces kinking, facilitating advancement and tamponade of tissue. The MPEC probe can be applied tangentially or perpendicularly to the bleeding source. Pressure is applied to compress and seal the walls of the bleeding vessel — a technique known as “coaptive coagulation” (3). MPEC probes are available in 7 Fr and 10 Fr diameters, each with an irrigation port at the tip; the 10 Fr probe requires an endoscope with a ≥3.2 mm instrument channel. Probe size, wattage, contact pressure, duration, and number of applications vary depending on the lesion being treated (2).
Indications and Technical Considerations
Although the injection gold probe is a valuable device in the endoscopic hemostasis armamentarium, it is not our first-line instrument — other highly effective options such as through-the-scope (TTS) clips or over-the-scope clips (OTSC) are often preferred. However, this case was ideally suited for the injection gold probe: the ulcer was located anteriorly — on the working channel side of the endoscope. When a duodenal ulcer is located posteriorly or on the right side of the endoscope, applying injection or gold probe therapy becomes technically challenging or impossible (3).
Complications and Safety Considerations
In our experience, we have not encountered significant complications with the gold probe. However, we have witnessed at least three cases of duodenal perforation at other institutions. Clinicians should therefore exercise caution during pressure hemostasis, as electrosurgical heat may cause thermal injury to deeper tissue layers (2, 4).
List of Abbreviations
EGD: esophagogastroduodenoscopy; MPEC: multipolar electrocoagulation; TTS: through-the-scope; OTSC: over-the-scope clip; UGIB: upper gastrointestinal bleeding; APC: argon plasma coagulation; Fr: French; NBVV: non-bleeding visible vessel
References
- Wasserman RD, Abel W, Monkemuller K, Yeaton P, Kesar V, Kesar V. Non-variceal Upper Gastrointestinal Bleeding and Its Endoscopic Management. Turk J Gastroenterol. 2024 May 20;35(8):599–608. doi: 10.5152/tjg.2024.23507. PMID: 39150279; PMCID: PMC11363156.
- Parsi MA, et al. Devices for endoscopic hemostasis of nonvariceal GI bleeding (with videos). VideoGIE. 2019;4:285–299.
- Treating Upper Gastrointestinal Bleeding: An Update on Endoscopic Techniques – EndoCollab.
- Kumar VCS, Aloysius M, Aswath G. Adverse events associated with the gold probe and the injection gold probe devices used for endoscopic hemostasis: A MAUDE database analysis. World J Gastrointest Endosc. 2024 Jan 16;16(1):37–43. doi: 10.4253/wjge.v16.i1.37. PMID: 38313458; PMCID: PMC10835479.
