
Case Report
Two cases of transient left-sided ischemic colitis are presented, highlighting the classic endoscopic features — including rectal sparing, segmental distribution, and Zuckerman’s sign — that are key to diagnosis.
Klaus Mönkemüller, MD, PhD, FASGE, FJGES
Virginia Tech Carilion School of Medicine, Virginia, USA
Dr. Mönkemüller is a Professor of Medicine and internationally recognized expert in advanced endoscopy. He has published over 400 peer-reviewed articles and is a Fellow of the American Society for Gastrointestinal Endoscopy (FASGE) and Fellow of the Japanese Gastroenterological Endoscopy Society (FJGES).
Troy Pleasant, MD
Virginia Tech Carilion School of Medicine, Virginia, USA
Dr. Pleasant is a gastroenterologist at Virginia Tech Carilion School of Medicine with clinical expertise in colonoscopy and lower gastrointestinal disorders.
Anand Dwivedi, MD
Virginia Tech Carilion School of Medicine, Virginia, USA
Dr. Dwivedi is a gastroenterologist at Virginia Tech Carilion School of Medicine specializing in inflammatory and ischemic bowel conditions.
Published: November 29, 2025
Abstract
Background: Transient or left-sided ischemic colitis is the most common type of ischemia of the gastrointestinal tract and the second or third most common cause of lower GI bleeding. It is characterized by acute onset abdominal pain and bloody diarrhea, predominantly affecting the left colon at watershed vascular zones.
Case Presentations: Two cases are presented: (1) an elderly patient with bloody diarrhea and patchy left-sided colitis on colonoscopy with histologic confirmation of ischemic colitis; and (2) a 60-year-old woman with hematochezia after acute left-sided abdominal pain, with CT showing left colonic stenosis and characteristic endoscopic findings.
Conclusion: Awareness of the classic endoscopic spectrum of ischemic colitis — rectal sparing, segmental distribution, Zuckerman’s sign, and watershed anatomy — is essential for accurate diagnosis and appropriate management.
Keywords: ischemic colitis; transient ischemic colitis; left-sided colitis; Zuckerman’s sign; colon single strip sign; lower GI bleeding; watershed areas; endoscopy
★ Key Clinical Takeaways
- Transient left-sided ischemic colitis is the most common GI ischemia and a leading cause of lower GI bleeding — the left colon at the watershed zones (Griffith’s and Sudeck’s points) is most vulnerable.
- Classic endoscopic findings include rectal sparing, segmental patchy erythema and edema, subepithelial hemorrhages, and the colon single strip sign (CSSS) — also known as Zuckerman’s sign.
- Key differential diagnoses include infectious colitis, diverticulitis, and inflammatory bowel disease; stool cultures (including for Klebsiella oxytoca and EHEC) and histology are essential to the workup.
- Risk factors include atherosclerosis, heart failure, arrhythmias, vasculopathies, aortic surgery, and hypercoagulability; medications such as estrogens, NSAIDs, and alosetron are classically associated.
- Most cases are self-limited and managed supportively; surgical resection is reserved for clinically unstable patients with peritonitis.
Introduction
Ischemic colitis is the most common form of gastrointestinal ischemia, accounting for approximately 1 in 1,000 hospital admissions and representing the second or third most frequent cause of lower gastrointestinal bleeding in adults over 60. The left colon — particularly the watershed areas at Griffith’s point (splenic flexure) and Sudeck’s point (rectosigmoid junction) — is disproportionately affected due to its tenuous blood supply at the margins of the superior and inferior mesenteric arterial territories.
The condition is frequently underdiagnosed or misclassified as inflammatory bowel disease or infectious colitis. Recognition of its characteristic endoscopic features — segmental distribution, rectal sparing, subepithelial hemorrhages, and the pathognomonic colon single strip sign (CSSS), also known as Zuckerman’s sign — is critical for prompt and accurate diagnosis. Herein we present two illustrative cases with a focus on the endoscopic spectrum of transient left-sided ischemic colitis.
Case Presentations
Case 1
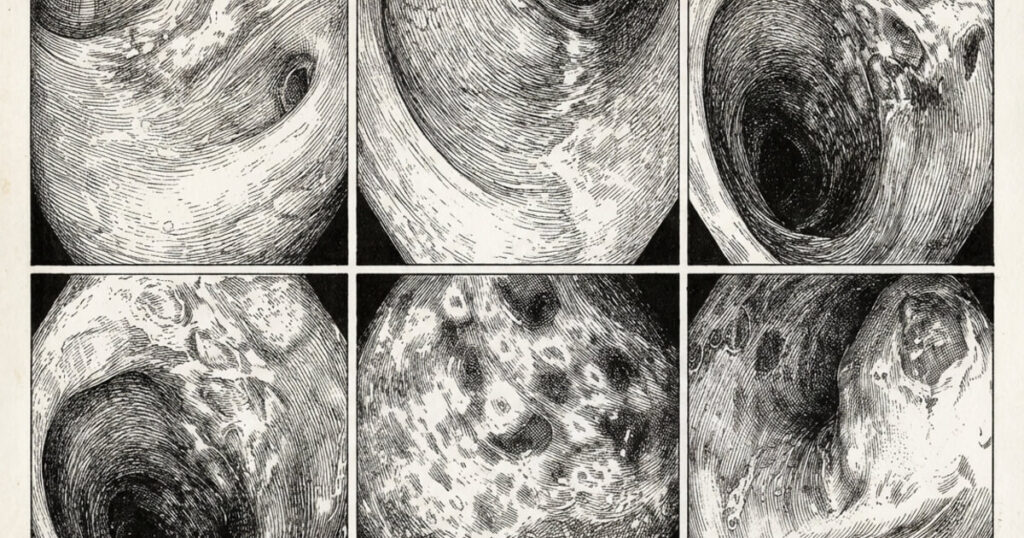
An elderly patient developed abdominal pain followed by bloody diarrhea. Colonoscopy showed patchy colitis of the left colon (Figure 1) with rectal sparing. Panel A shows small ulcers with an erythematous halo. In Panels C to E, the classic Zuckerman sign can be appreciated.

A diagnosis of ischemic colitis was confirmed histologically. There were no significant risk factors for vascular occlusive disease or vasculitis. The patient improved with supportive measures and was discharged home two days later.
Case 2
A 60-year-old female patient without significant past medical history presented with hematochezia that started after acute onset left-sided abdominal pain. Only the bleeding continued; the pain disappeared after approximately 12–18 hours. CT of the abdomen revealed left-sided colon stenosis and inflammation. Colonoscopy images are shown in Figure 2.

Discussion
Colonic ischemia occurs due to changes in systemic circulation and/or alterations in local mesenteric vasculature. Left-sided ischemic colitis, also called transient ischemic colitis, is characterized by acute onset abdominal pain and bloody diarrhea or hematochezia. This condition can occur in any age group, but is most commonly seen in the elderly. Risk factors include atherosclerosis, heart failure, cardiac arrhythmias, shock, vasculopathies, abdominal aortic surgery, and hypercoagulability states. Abrupt changes in blood flow — such as those occurring after a marathon, exertion, or transient vessel occlusion from constriction (cocaine), thrombosis, or low flow state — can also result in transient ischemic colitis. Classic medications associated with ischemic colitis include estrogens, NSAIDs, and alosetron (1).
The most frequently affected areas are the left colon and superior rectum; the lower rectum is usually spared because of its dual blood supply. The main differential diagnoses are infectious colitis, diverticulitis, and inflammatory bowel disease. Stool cultures and histology are an important part of the workup. Standard stool cultures do not detect Klebsiella oxytoca or enterohaemorrhagic Escherichia coli — this should be specifically stated in the microbiology request. The diagnosis is established by endoscopy and histology (1).
The endoscopic spectrum of ischemic colitis is broad (Figure 3).

Key elements include sparing of the rectum and segmental distribution, mainly in the left colon at the watershed area (arc of Riolan). These watershed zones are known as Sudeck’s and Griffith’s points (Figure 4).

In mild ischemic colitis, there are typically segmentally distributed patchy erythema, edema, and subepithelial hemorrhages. In moderate colitis, additional localized erosions and ulcers may be confluent. A linear ulcer along the mesenteric border of the colon — the colon single strip sign (CSSS) or Zuckerman’s sign — is often present (1). In severe colitis, deep ulcers, luminal narrowing, strictures, and frank necrosis are seen.

Most cases of ischemic colitis are self-limited and do not require specific medical or surgical therapy. However, in clinically unstable patients with signs of peritonitis, colon resection should be considered.
Conflict of Interest
No conflicts of interest declared by KM, TP, or AD with any of the companies, utensils, or products mentioned in this article.
How to Cite
Mönkemüller K, Pleasant T, Dwivedi A. Transient or “Left”-Sided Ischemic Colitis: Case Reports With Focus on its Endoscopic Spectrum. EndoCollab. November 29, 2025. Available at: https://endocollab.com/blogs/gi-endoscopy-tips-tricks/transient-or-left-sided-ischemic-colitis-case-reports-with-focus-on-its-endoscopic-spectrum/
References
- Monkemüller K, Wilcox CM. Ischemic Colitis. VideoGIE. 2014. Available at: https://www.videogie.org/article/S2212-0971(13)70152-3/fulltext
- Lecturio Medical. Mesenteric Ischemia. Available at: https://www.lecturio.com/concepts/mesenteric-ischemia/
