
Case Report
![]() Klaus Mönkemüller, MD, PhD, FASGE, FESGE, FJGES
Klaus Mönkemüller, MD, PhD, FASGE, FESGE, FJGES
Professor of Medicine, Department of Gastroenterology, Carilion Memorial Hospital, Virginia Tech Carilion School of Medicine, Roanoke, USA
Experienced teaching points
Clinical Pearls
01Guidewire placement is critical for safe endoscopic balloon dilation of duodenal stenoses, preventing distal perforation.
02Direct endoscopic visualization during balloon inflation allows for real-time monitoring of mucosal changes.
03Water can be an effective and practical inflation medium for balloon dilation without fluoroscopy.
04Post-dilation endoscopic inspection confirms successful stenosis widening and identifies any immediate complications.
Get cases like this every other Saturday. Free on The Practicing Endoscopist.
Clinical History
A 75-year-old male presented with nausea, vomiting, and abdominal distension. A computed tomography scan of the abdomen confirmed gastric outlet obstruction. Endoscopy was indicated to evaluate and manage the obstruction.

Endoscopic Findings
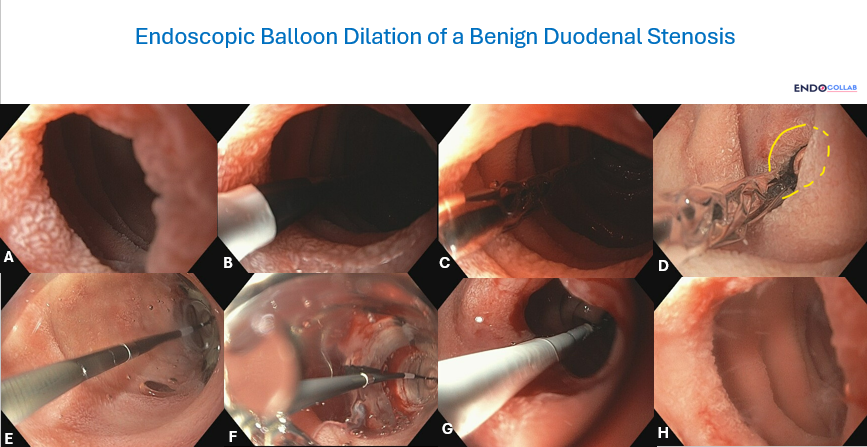
A ring-like fibroinflammatory stenosis was identified between the first and second portions of the duodenum (Panel A). The stenosis was approximately 5 mm thick and 8 mm in diameter. The gastroscope could not pass through the stenosis.
Endoscopic Technique
A guidewire was advanced through the stenosis. A through-the-scope, controlled radial expansion balloon dilation catheter was advanced over the guidewire (Panel B). A 13-14-15 mm balloon catheter was positioned such that the first marker was visible, and then pulled back to ensure approximately half the length of the balloon was across the stenosis (Panels C, D) for homogeneous dilation.
The balloon was inflated with water (Panel E) under direct endoscopic visualization, observing mucosal rips (Panel F). Post-dilation inspection (Panel G) was performed by advancing the deflated balloon deep into the dilated area. Mucosal breaks were even and not deep (Panel H). The endoscope could easily pass through the post-dilation stenosis.
Discussion
Endoscopic balloon dilation is a safe and effective technique for benign duodenal stenoses, particularly when a guidewire is utilized to prevent distal perforation. Visualizing mucosal rips during dilation provides real-time feedback on the adequacy of dilation and helps prevent over-dilation.
The use of water for balloon inflation in cases without fluoroscopic guidance offers smoother and easier inflation compared to contrast medium. A final inspection with the balloon catheter after deflation confirms successful dilation and assesses for complications.
References
- Adler DG, Baron TH, Mashimo R, et al. Endoscopic balloon dilation of gastrointestinal stenoses: methodology and future directions. Gastrointest Endosc. 2004;60(1):151-155.
- Standards of Practice Committee, ASGE. The role of endoscopy in the management of benign adult esophageal strictures. Gastrointest Endosc. 2021;93(3):525-538.
- Kim M, Kim SJ, Lee TH, et al. Endoscopic balloon dilation for benign anastomotic stricture after gastric cancer surgery. BMC Gastroenterol. 2018;18(1):157.
For your teaching file
Save this case as a PDF
Opens the companion page on The Practicing Endoscopist.



