
Case Report
![]() Klaus Mönkemüller, MD, PhD, FASGE, FESGE, FJGES
Klaus Mönkemüller, MD, PhD, FASGE, FESGE, FJGES
Professor of Medicine, Department of Gastroenterology, Carilion Memorial Hospital, Virginia Tech Carilion School of Medicine, Roanoke, USA
Experienced teaching points
Clinical Pearls
01Self-expanding metal stents serve as an effective bridge to surgery for decompression of benign colonic obstructions, such as those caused by diverticulitis.
02Combined endoscopic and fluoroscopic guidance is crucial for safe and accurate guidewire placement and stent deployment.
03Utilizing a transparent distal cap facilitates visualization and scope stabilization when navigating stenotic segments.
04Careful attention to stent-specific deployment mechanisms, such as markers and migration tendencies, is essential for successful placement.
05Stent placement allows for bowel decompression and improved surgical conditions, potentially avoiding emergent colostomy.
Get cases like this every other Saturday. Free on The Practicing Endoscopist.
Clinical History
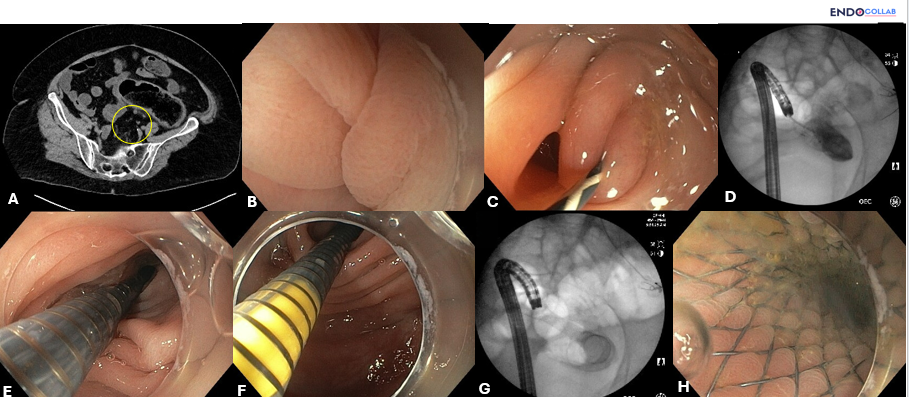
A 72-year-old female presented with abdominal pain, distention, nausea, and vomiting. A computed tomography scan of the abdomen demonstrated acute sigmoid diverticulitis with partial bowel obstruction and a significant amount of retained stool. The patient had several previous episodes of diverticulitis. Surgical intervention was considered necessary. However, given the bowel obstruction, the risks of emergency surgery were increased, and a colostomy would be mandatory. Therefore, a decision was made to place a self-expanding metal stent to decompress the obstruction and serve as a bridge to surgery.

Endoscopic Findings
A stenotic sigmoid colon due to severe diverticulitis was identified. The stenosis prevented passage of the therapeutic scope.
Endoscopic Technique
The placement of the self-expanding colonic metal stent began with the determination of the stricture site (Panel B). A therapeutic gastroscope with a 3.7 mm working channel was utilized, fitted with a distal transparent cap to retract mucosal folds, stabilize the scope tip, and focus on the lumen.
Upon encountering the stenosis, a 0.035-inch guidewire (Panel C) was advanced through the scope using a balloon catheter, guided by combined endoscopy and fluoroscopy (Panel D). Once the guidewire was confirmed to be safely positioned within the colonic lumen proximal to the stricture, contrast was injected through the catheter, confirming the luminal position. The catheter was then removed, leaving the guidewire in place.
An Evolution non-covered self-expanding metal stent (Cook Medical, USA) was advanced over the guidewire, through the scope, and across the stricture (Panel E). Deployment of the stent was guided by fluoroscopic visualization of the expanding stent and endoscopic visualization of the delivery device (Panels F, G). The Evolution self-expanding metal stent has a yellow delivery catheter below the stent, which was continuously visualized during deployment (Panel F). As the stent tends to migrate proximally during deployment, constant traction on the stent delivery device was maintained to ensure a stable position. Monitoring the yellow marker was essential to guarantee proper deployment of the distal flange of the self-expanding metal stent distal to the stricture (Panels F, G, H).
The patient had an uneventful post-endoscopy course and will undergo elective surgery once the colon has been decompressed and adequately prepped, thus avoiding complications and a colostomy.
Discussion
This case highlights the utility of uncovered self-expanding metal stents for decompression of colonic obstruction, particularly in the setting of acute diverticulitis with partial bowel obstruction. The use of a stent as a bridge to surgery allowed for bowel decompression and preparation, thus potentially reducing the need for an emergent colostomy and mitigating surgical risks associated with operating on an unprepared, obstructed colon.
The technique emphasized precise guidewire placement under combined endoscopic and fluoroscopic guidance, and careful stent deployment with attention to the unique features of the stent delivery system, such as the yellow catheter marker and the tendency for proximal migration, to ensure optimal positioning and prevent complications. This approach demonstrates that self-expanding metal stents can be effectively used for benign conditions causing colonic stenosis, such as diverticulitis, in addition to their more common application in malignant obstructions. For more insights on stenting options in benign stenoses, see our discussion on fully covered metal stents for duodenal stenosis.
References
- van Hooft JE, van Halsema EE, Baron TH, et al. Self-expanding metal stents for obstructing benign colonic strictures: a systematic review. Endoscopy. 2012;44(6):581-591.
- Lamazza A, et al. Self expandable metal stents for left-sided colon obstruction from diverticulitis. A single center experience. Medicina (Kaunas). 2021;57:299.
For your teaching file
Save this case as a PDF
Opens the companion page on The Practicing Endoscopist.



