
CASE REPORT
Abstract
Background: Esophageal inlet patches are areas of ectopic gastric mucosa found in the upper esophagus, present in approximately 3–5% of patients undergoing upper endoscopy. While most are asymptomatic, inlet patches can cause dysphagia, globus sensation, and rarely esophageal stricture formation leading to food impaction.
Case: A 52-year-old woman presented with acute dysphagia. Upper endoscopy revealed a 20 × 30 mm esophageal inlet patch, a distal fibrotic stricture, and a piece of impacted chicken meat in the midesophagus with an additional stricture distally. The impacted food was removed using a distal transparent cap. The patient was started on proton pump inhibitors, and subsequent endoscopy with esophageal dilation up to 16 mm was performed.
Conclusion: This case illustrates an uncommon but clinically significant presentation of an esophageal inlet patch causing stricture formation and acute food impaction. Recognition of inlet patches as a potential cause of esophageal strictures is important for appropriate management, including endoscopic dilation, acid suppression, and consideration of ablative therapy.
Keywords: esophageal inlet patch; heterotopic gastric mucosa; cervical inlet patch; food impaction; esophageal stricture; dysphagia; endoscopic dilation; argon plasma coagulation; proton pump inhibitors; ectopic gastric mucosa
★ Key Clinical Takeaways
- Esophageal inlet patches are present in 3–5% of patients undergoing upper endoscopy; most are asymptomatic, but they can cause dysphagia, globus sensation, cough, and hoarseness when symptomatic.
- Inlet patches should be considered in the differential diagnosis of proximal esophageal strictures — acid secretion from ectopic gastric mucosa can cause chronic inflammation and fibrotic narrowing.
- Food impaction in the setting of an inlet patch-associated stricture requires endoscopic foreign body removal followed by esophageal dilation and acid suppression therapy.
- Proton pump inhibitors reduce acid secretion from ectopic gastric mucosa and should be initiated in symptomatic patients; ablative therapies such as argon plasma coagulation or radiofrequency ablation are effective for definitive treatment.
- During upper endoscopy, careful inspection of the proximal esophagus immediately below the upper esophageal sphincter is essential — inlet patches are easily missed with rapid scope advancement.
Clinical History
A 52-year-old woman presented with acute dysphagia. She had no significant prior gastrointestinal history. Upper endoscopy was performed to evaluate the cause of her symptoms.
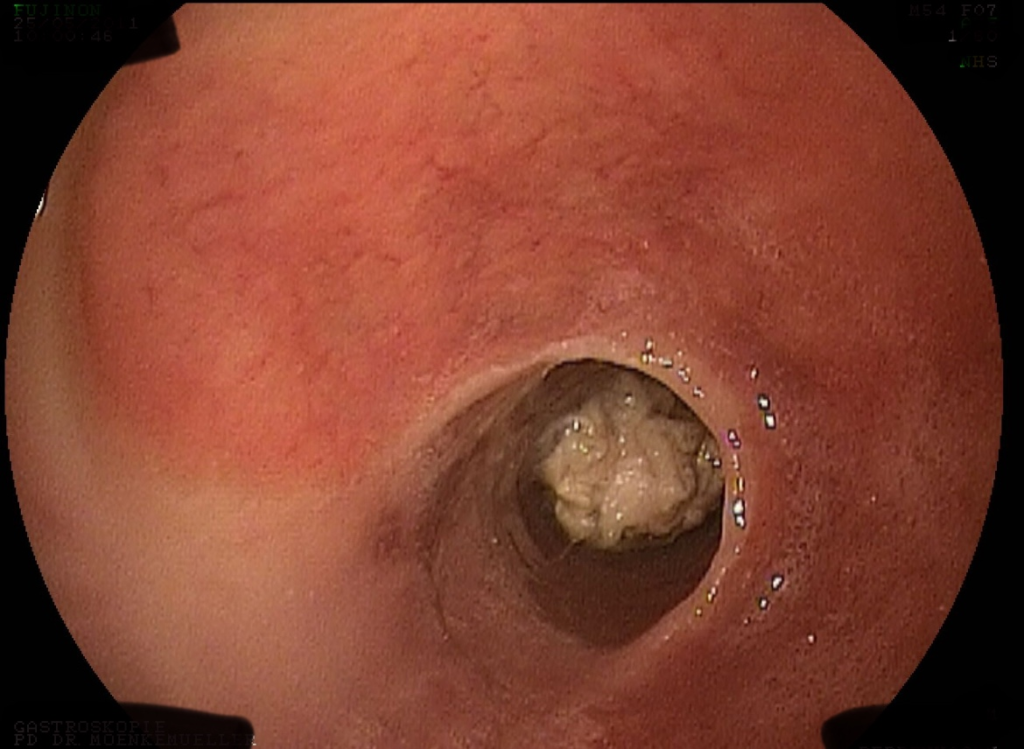
Endoscopic Findings
During upper endoscopy, a large esophageal inlet patch measuring 20 × 30 mm was identified in the upper esophagus. A distal fibrotic stricture was noted in the esophagus. Distal to the fibrotic stricture, a piece of chicken was impacted in the midesophagus. An additional esophageal stricture was observed distal to the food impaction.

Endoscopic Technique
The impacted chicken meat was removed using a distal transparent cap attached to the endoscope. Following the initial procedure, the patient was initiated on proton pump inhibitors. A subsequent upper endoscopy was performed where esophageal dilation was carried out up to 16 mm.
Discussion
An inlet patch, also known as esophageal heterotopic gastric mucosal patch or cervical inlet patch, is a common but often overlooked area of ectopic gastric mucosa found in the upper esophagus. It is present in approximately 3 to 5% of patients undergoing upper endoscopy. While most patients are asymptomatic, some may experience symptoms such as dysphagia, cough, globus sensation, or hoarseness.
Treatment for symptomatic inlet patch involves ablating the tissue, typically using techniques like argon plasma coagulation or radiofrequency ablation. Proton pump inhibitors are beneficial in reducing acid secretion from the ectopic gastric mucosa. Moreover, patients with associated esophageal strictures, as in this case, benefit from endoscopic dilation.
This case highlights an uncommon presentation of an inlet patch causing esophageal stricture and acute food impaction.
References
- Behrens C, Yen NPP. Esophageal patch. Radiology Research and Practice. 2011;2011:2460890.
- Bindlish S, Murali R. Inlet patch stricture: a case report. American Journal of Gastroenterology. 2010;105:23.
- Bajbouj M, et al. Argon plasma coagulation of cervical heterotopic gastric mucosa as an alternative treatment for globus sensation. Gastroenterology. 2009;137:440–4.
