
CASE REPORT
Abstract
Background: Ileal neuroendocrine tumors (carcinoid tumors) are slow-growing neoplasms arising from enterochromaffin cells that account for approximately 28% of terminal ileal carcinoids. They are frequently diagnosed late due to non-specific symptoms, and metastasis to the liver and lymph nodes may have already occurred at the time of diagnosis.
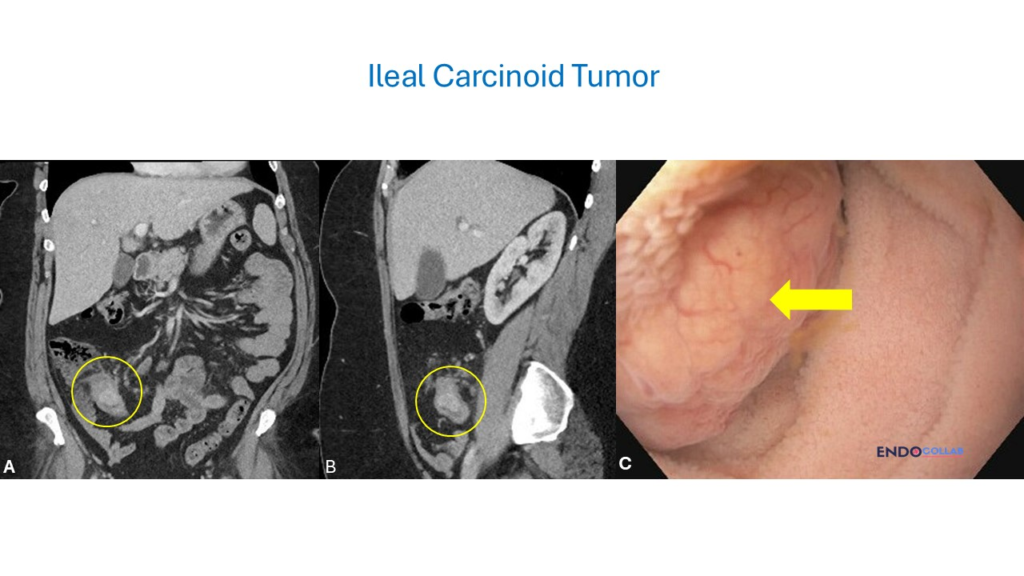
Case: A 54-year-old woman presented with two weeks of abdominal pain and a history of chronic constipation. CT imaging revealed a 2.6 cm hyperenhancing, pedunculated-appearing lesion in the terminal ileum with adjacent soft tissue thickening and no lymph node enlargement. Ileocolonoscopy identified a large, partially lumen-obstructing mass approximately 3 cm in size, located 4–5 cm from the ileocecal valve. The lesion appeared yellowish, firm, and polypoid with superficial vessels. Biopsies confirmed a neuroendocrine tumor with G1 differentiation.
Conclusion: This case highlights the importance of cross-sectional imaging in the incidental discovery of ileal neuroendocrine tumors and the characteristic endoscopic features — yellowish color, firm consistency, polypoid morphology — that should raise suspicion for carcinoid. Early identification is critical given the risk of metastasis and carcinoid syndrome.
Keywords: ileal carcinoid; neuroendocrine tumor; terminal ileum; colonoscopy; CT imaging; carcinoid syndrome; enterochromaffin cells; small bowel neoplasm
★ Key Clinical Takeaways
- Ileal neuroendocrine tumors frequently present with non-specific abdominal pain, making cross-sectional imaging essential for early detection — most early carcinoids are asymptomatic.
- On endoscopy, characteristic features include a yellowish, firm, polypoid lesion with superficial vessels and submucosal location; these features should immediately raise suspicion for carcinoid.
- CT imaging identified a 2.6 cm hyperenhancing pedunculated lesion in the terminal ileum — the hyperenhancing pattern on CT is a hallmark of neuroendocrine tumors.
- Advanced carcinoid syndrome (flushing, diarrhea, sweating) occurs in approximately 10% of cases, typically after hepatic metastasis, and carcinoid heart disease (tricuspid valve damage) is a rare but serious complication.
- Biopsy confirmation with histological grading (G1/G2/G3) is mandatory for treatment planning; direct tissue visualization via colonoscopy, capsule endoscopy, or deep enteroscopy with biopsies provides definitive diagnosis.
Clinical History
A 54-year-old woman presented with two weeks of abdominal pain. She had a history of chronic constipation but was otherwise healthy. Given her new symptoms, a CT scan of the abdomen and pelvis was obtained. The CT scan identified a 2.6 cm hyperenhancing, pedunculated-appearing lesion within the terminal ileum with adjacent right lower quadrant soft tissue thickening and no lymph node enlargement, concerning for a neoplasm.
Endoscopic Findings
During ileocolonoscopy, a large and partially lumen-obstructing mass was observed, measuring approximately 3 cm and located 4 to 5 cm from the ileocecal valve. The lesion appeared rounded and polypoid, with a yellowish color, a smooth surface with multiple superficial vessels, and was firm to the touch with the biopsy forceps.

Endoscopic Technique
A colonoscopy was performed with intubation of the terminal ileum. Eight biopsies were obtained from the ileal lesion using biopsy forceps. Histology confirmed a neuroendocrine tumor with G1 differentiation. No complications occurred during the procedure.
Discussion
Carcinoid or neuroendocrine tumors are slow-growing neoplasms arising from enterochromaffin cells in the small intestine. They account for approximately 28% of terminal ileal carcinoids. These tumors are frequently diagnosed late due to non-specific symptoms such as abdominal pain or diarrhea, at which point metastasis to the liver and lymph nodes may have already occurred. Most early carcinoids are asymptomatic, though patients may experience intermittent abdominal pain, nausea, and some weight loss.
In the presented case, the incidental discovery on CT imaging led to the early recognition of this lesion. Advanced carcinoid syndrome occurs in about 10% of cases, commonly after metastasis, and is characterized by flushing, chronic watery diarrhea, and sweating.
Common complications of ileal carcinoids include small bowel obstruction and intestinal bleeding. Rarely, tricuspid cardiac valve damage (carcinoid heart disease) occurs, but only in the setting of metastatic disease.
Diagnostic tests for ileal carcinoid include CT or MRI scans of the abdomen and pelvis, serum blood tests such as chromogranin A, 24-hour urine for 5-hydroxyindoleacetic acid, and somatostatin receptor imaging (Octreoscan or PET/CT). Obtaining direct tissue visualization via capsule endoscopy or deep endoscopy, such as single or double-balloon enteroscopy with biopsies, is crucial for histological confirmation of the disease.
References
- Gaujoux S, Itzkowitz SH. Ileal carcinoid tumors. Gastroenterology. 2009;137(3):805-809.
- Kulke MH. Carcinoid tumors. Curr Opin Oncol. 2006;18(1):52-57.
- Ramage JK, Ahmed A, Ardill J, et al. Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours (NETs). Gut. 2012;61(1):6-32.
