
by Hiral Patel, MD and Klaus Klaus Mönkemüller, MD, PhD, FASGE, FJGES
Department of Gastroenterology, Carilion Memorial Hospital, Virginia Tech Carilion School of Medicine, Roanoke, USA
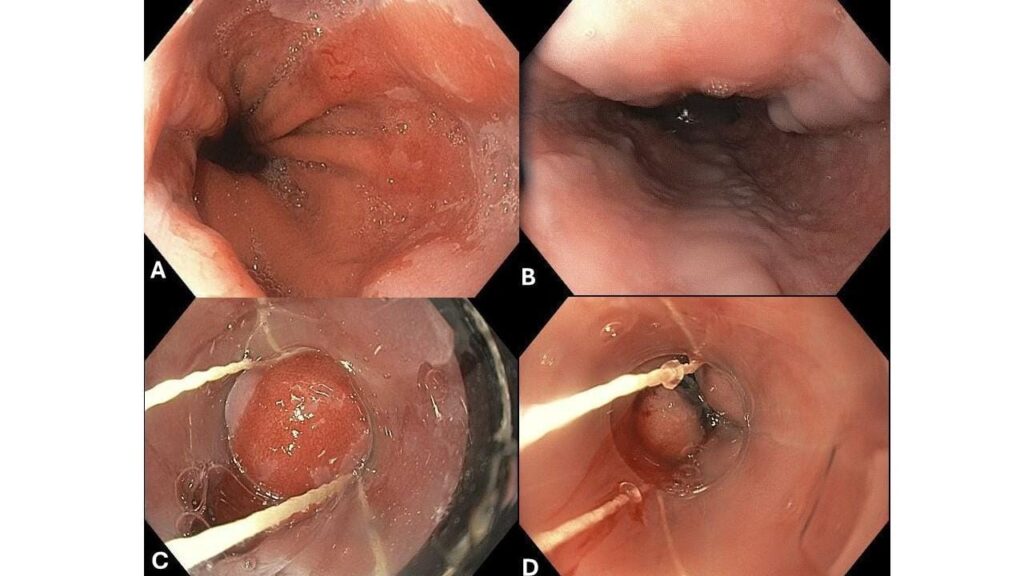
A 50-year-old patient was sent to our endoscopy service because of Barrett’s esophagus and esophageal varices.
He had been biopsied at another institution for a tongue of cylindrical epithelium in the distal esophagus. Before going into the discussion on the approach to this case we want to emphasize that one should never biopsy lesions in the setting of esophageal or gastric varices unless there is a backup plan for the obliteration of the bleeding.
In this case, we decided to band the segment of Barrett’s mucosa (Figures 2C and 2D). This approach was first reported by Diaz-Cervantes (1) and since then replicated and confirmed by other experts (2, 3).

In this case we decided to band the segment of Barrett’s mucosa (Figures 2C and 2D). This approach was first reported by Diaz-Cervantes (1) and since then replicated and confirmed by other experts (2, 3).

The initial idea of using endoscopic band ligation for Barrett in the setting of esophageal varices is Diaz-Cervantes from Mexico (1). In this study 30 patients with Barrett esophagus were treated with endoscopic band ligation plus omeprazole 20 mg t.i.d. endoscopic band ligation was repeated monthly until two consecutive endoscopic and histological examinations showed no BE. Thirty Barrett’s patients treated with omeprazole 20 mg t.i.d. alone served as a control group (1). The endoscopic band ligation treatment group comprised 29 patients with short-segment BE (SSBE) and one with long-segment disease, whereas all 30 of the control patients had SSBE. During a median follow-up of 16.9 months (range 10-24 months), complete eradication of Barrett’s esophagus was achieved in 29 of 30 patients (97%) in the endoscopic band ligation group. In contrast, Barrett’s esophagus persisted in all 30 control patients during the same period (P < 0.0005). The mean total number of bands applied per patient was 6.1 (range 1-14) and the mean number of sessions for complete eradication was 3.1 (range 1-7). Adverse events included only mild chest pain and dysphagia that resolved within days (1).
In a retrospective study from the USA, Hartgnik et al present eight cases of Barrett esophagus and esophageal varices that were successfully treated with band ligation alone (2). There was no bleeding, perforation or infectious complications in any patients undergoing banding for treatment of BE. Four patients had biopsy-proven dysplasia prior to treatment with band ligation. After band ligation, 2 of 4 dysplastic cases that had repeat biopsies showed histologic resolution of the dysplasia. All patients who received banding for BE were followed at least yearly except for one patient lost to follow-up. No interval esophageal cancers were reported in any patients with BE that were banded (2).
In a retrospective comparative study from the Mayo Cinic in Jacksonville, Florida eight high-grade dysplasia patients with varices who were treated initially with band-ligation were compared with reference group of 52 high-grade dysplasia patients treated endoscopically. A complete remission of intestinal metaplasia or dysplasia was obtained in 50% patients of with Barrett’s and varices. In the reference group (ablative therapies using heat and/or RFA) the disappearance of dysplasia and intestinal metaplasia was higher (75%) (3). Finally, Hadley et al (4) reported on a complete cure of an early esophageal adenocarcinoma overlying a varix, which was treated by endoscopic band ligation (4).
Of course, eradication of dysplastic Barrett esophagus makes sense. Whether eradication of non-dysplastic Barrett esophagus in the setting of esophageal varices should be performed routinely is a matter of debate. However, we believe that eradication of non-dysplastic Barrett esophagus in the setting of esophageal varices makes sense for two reasons: a) the follow-up endoscopies of BE with persistent varices may be avoided, and b) eradication of varices is associated with less risk of bleeding.
In sum, we believe that knowledge of this relatively safe technique, which is supported by various publications is an important addition to the therapeutic armamentarium of Barrett’s esophagus and even small early esophageal adenocarcinomas help deal with the dilemma of Barrett’s esophagus in the context of esophageal varices.
Want the PDF of this article? Reply to this email with “PDF” and we will send you the PDF file.
A big thank you to this week’s sponsor who helps keep this newsletter free for the reader:
EndoCollab. EndoCollab is an online community for GI endoscopists. With 1300+ members, endoscopists discuss interesting cases, view on-demand video courses, and get new endoscopy tips every day. Join EndoCollab
VIDEO OF THE WEEK
Endoscopic Therapy for Esophageal and Gastric Varices

Are you prepared to manage the high mortality and alarming recurrence rates of bleeding esophageal and gastric varices? These cases are critical and demand the most effective therapeutic approach.
This week’s “From My Toolbox” session with Dr. Mönkemüller cuts to the chase, giving you a clear overview of endoscopic therapy, and new developments for managing these high-risk patients.
Here’s what you’ll uncover:
The grim reality: Understand the mortality rates and recurrent bleeding risks associated with untreated esophageal/gastric varices (it’s higher than you think!)
The Pathophysiology: A breakdown of the natural history of the formation of esophageal and gastric varices.
Ligation vs. Sclerotherapy: Decide on the best therapy options: Understand why endoscopic variceal ligation surpasses sclerotherapy for emergency scenarios.
Don’t let valuable clinical time slip away. Stay ahead of the curve with the latest approaches in treating these life-threatening conditions.
Click here to watch “Endoscopic Therapy for Esophageal and Gastric Varices” now!
References:
1. Diaz-Cervantes E, De-la-Torre-Bravo A, Spechler SJ, Torres-Durazo E, Sobrino-Cossio S, Martínez-Carrillo O, Gamboa-Robles J. Banding without resection (endoscopic mucosal ligation) as a novel approach for the ablation of short-segment Barrett’s epithelium: results of a pilot study. Am J Gastroenterol. 2007 Aug;102(8):1640-5. doi: 10.1111/j.1572-0241.2007.01256.x. Epub 2007 May 3. PMID: 17488252.
2. Hartgerink C, Nimri FM, Zuchelli T, Jafri SM, Piraka C. Band Ligation Can Be Used to Treat Barrett’s Esophagus and Concurrent Esophageal Varices: A Case Series. Dig Dis Sci. 2023 Apr;68(4):1381-1385. doi: 10.1007/s10620-022-07696-1. Epub 2022 Sep 21. PMID: 36131048.
3. Palmer WC, Di Leo M, Jovani M, Heckman MG, Diehl NN, Iyer PG, Wolfsen HC, Wallace MB. Management of high grade dysplasia in Barrett’s oesophagus with underlying oesophageal varices: A retrospective study. Dig Liver Dis. 2015 Sep;47(9):763-8. doi: 10.1016/j.dld.2015.05.009. Epub 2015 May 21. PMID: 26066379
4. Hadley SM Jr, Patel NJ, Gardner TB. Band Ligation Resolves Esophageal Adenocarcinoma Overlying Esophageal Varix. ACG Case Rep J. 2022 Sep 1;9(9):e00823. doi: 10.14309/crj.0000000000000823. PMID: 36072356; PMCID: PMC9439847.
No COI by HP or KM with any of the companies/utensils or products mentioned in this article.
