
Dieulafoy Lesion of the Duodenum
Klaus Mönkemüller, MD, PhD, FASGE, FJGES
Department of Gastroenterology, Carilion Memorial Hospital, Virginia Tech Carilion School of Medicine, Roanoke, USA
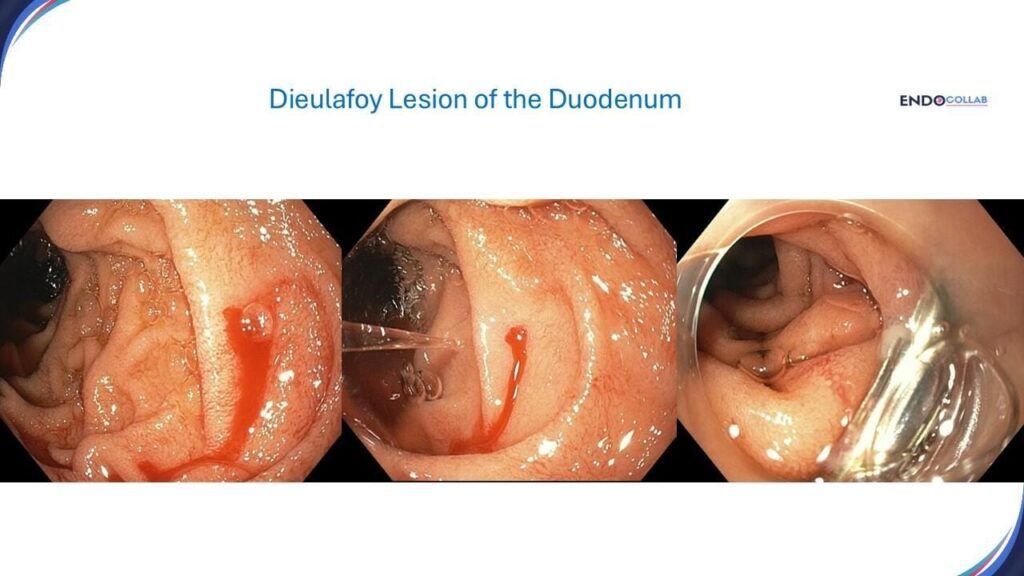
An 72-year-old female with past medical history of chronic kidney disease stage IV, type 2 diabetes mellitus, atrial fibrillation presented with recurrent overt gastrointestinal bleeding (melena and hematemesis, hemoglobin 7.1 gr/dl). She had undergone two previous EGDs without significant findings. On EGD we found a bleeding Dieulafoy lesion of the duodenum (Figure 1). Hemostasis achieved with a hemoclip.

Figure 1. Dieulafoy lesion of the duodenum. A. Active bleeding. B. No evidence of ulceration or angiodysplasia. C. Successful hemostasis with a through-the-scope clip.
A Dieulafoy lesion is a rare, developmental vascular malformation in the gastrointestinal (GI) tract that can cause bleeding (1). This enlarged and erratic submucosal blood vessel may bleed in the absence of any visible abnormality, such as ulcers or erosions (1). However, on histology the vessel often results in an erosion of the mucosa, hence its classic name “exulceratio simplex” (2). Other names for Dieulafoy are cirsoid aneurysm and caliber-persistent submucosal vessel (1). A Dieulafoy lesion can occur anywhere in the GI tract, but most often in the stomach. This lesion is more common in males, the average age is 70 years. The most common symptoms are unexplained, recurrent, or massive GI bleeding. Dieulafoy lesion accounts for 6.5% of the causes of upper gastrointestinal hemorrhage (3). Therapy is mainly endoscopic, including epinephrine injection, electrocoagulation, or clip placement (1). In cases of severe bleeding, angiogram with selective embolization is an excellent option. Rarey, surgical resection may be necessary as a last resort.
References:
1. Malik TF, Anjum F. Dieulafoys Lesion Causing Gastrointestinal Bleeding. StatPearls Publishing; 2025 Jan-.
2. Dieulafoy G. Exulceratio simplex: leçons 1–3. In: Dieulafoy G, editor. Clinique Médicale de l’Hotel Dieu de Paris. Paris, France: Masson et Cie; 1898. pp. 1–38.
3. Then EO, Bijjam R, Ofosu A, Rawla P, Culliford A, Gaduputi V. Rectal Dieulafoy’s Lesion: A Rare Etiology of Lower Gastrointestinal Hemorrhage. Case Rep Gastroenterol. 2019 Jan-Apr;13(1):73-77
